Full Text Hide / show
Background
:Antimicrobial resistance (AMR) is a global public health threat, with hospital wastewater increasingly recognized as an environmental reservoir of antibiotic residues, resistant bacteria, and resistance genes. In resource-limited settings such as Lubumbashi (Democratic Republic of Congo), inadequate wastewater treatment may contribute to environmental dissemination of resistant strains. Objective: To evaluate hospital effluent management and assess its role in reducing the risk of environmental transmission of antibiotic-resistant bacteria. Methods: An analytical cross-sectional study was conducted in public and private hospitals in Lubumbashi. Data were collected on antibiotic disposal practices, wastewater treatment systems, environmental monitoring, and staff training. An Effluent Management Score (EMS) was developed. Bivariate analyses and multivariate logistic regression were performed to identify factors associated with high environmental transmission risk.
Model performance was assessed using ROC curve analysis. Results: Fewer than 25% of hospitals had specific wastewater treatment systems, and environmental monitoring was performed in less than 10% of facilities. Lack of wastewater treatment (OR = 4.52; p < 0.001), absence of an internal treatment plant (OR = 3.78; p < 0.001), uncontrolled antibiotic disposal (OR = 3.21; p = 0.004), lack of environmental monitoring (OR = 4.01; p < 0.001), and absence of staff training (OR = 2.87; p = 0.008) were significantly associated with high risk. Each one-point increase in EMS reduced risk by 38% (aOR = 0.62; p < 0.001). The model demonstrated good discrimination (AUC = 0.83).
Conclusion
: Poor hospital wastewater management significantly increases environmental AMR transmission risk. Strengthening effluent treatment, monitoring, and staff training represents a strategic environmental lever within a One Health framework. Keywords: Antimicrobial resistance; Hospital wastewater; Antibiotic residues; Environmental transmission; One Health.
Introduction
Antibiotic resistance is a global health threat that extends beyond the strictly clinical setting to include the environment as a reservoir and vector for the spread of resistant bacteria[1]. Among the most concerning environmental sources are hospital effluents , which contain antibiotic residues, pathogenic bacteria, and resistance genes[2,3]. In hospitals, a significant proportion of antibiotics administered to patients are excreted in active or partially metabolized form[4-6]. These residues are then discharged into wastewater systems without adequate treatment in many resource-limited countries[7-9]. Hospital wastewater thus becomes a favorable environment for the selection, persistence, and spread of resistant bacterial strains[7,10-12]. In Lubumbashi, inadequate hospital wastewater treatment systems, combined with the intensive use of antibiotics, expose the environment and the population to an increased risk of antibiotic resistance transmission.
Proper management of hospital wastewater therefore appears to be a key environmental lever in the fight against antibiotic resistance [13,14]. This study aims to analyze the management of antibiotic residues in hospital effluents and to evaluate its role in preventing the transmission of antibiotic-resistant strains. STUDY OBJECTIVES General objective Evaluate the management of antibiotic residues in hospital effluents as a means of combating the transmission of antibiotic-resistant strains in Lubumbashi. Specific objectives • Describe hospital effluent management practices; • Identify the sources and factors of contamination by antibiotic residues; • Evaluate the existence and effectiveness of effluent treatment systems; • Analyze the link between poor effluent management and the risk of antibiotic resistance; • To propose environmental strategies to combat antimicrobial resistance.
Methodology
Type and framework of the study Analytical cross-sectional observational study conducted in public and private hospitals in the city of Lubumbashi. Population and units of analysis • Hospital services that use antibiotics; • Liquid waste (effluent) management systems; • Hospital managers and technical staff. Calculating the minimum size Unit of analysis: hospital settings. Variable: high risk of environmental transmission. In the absence of known prevalence: n=384 However, if the hospital population is limited (e.g., 120 establishments), a finite population correction is applied: ncorrige = If N = 120: ncorrige ≈92 Estimated minimum size: 90–100 establishments Inclusion criteria • Public or private hospitals • Regular use of antibiotics • Existing wastewater disposal system • Administrative authorization obtained Exclusion criteria • Outpatient centers • Structures without antibiotic activity • Institutional refusal • Environmental data unavailable Variables studied Dependent variable • Risk of transmission of resistant strains via effluents (presumed/high vs low).
Independent variables • Presence of antibiotic residues in the effluents; • Existence of an effluent treatment system; • Type of treatment (none, primary, secondary); • Compliance with environmental standards; • Raising awareness among hospital staff. Data analysis • Descriptive analysis (frequencies, percentages); • Bivariate analysis (OR, Chi-square); • Logistic regression to identify factors associated with a high risk of dissemination of resistance. methodological justification The choice of an analytical cross-sectional observational design is justified by the objective of this study, which aims to evaluate hospital effluent management practices and identify factors associated with the risk of environmental transmission of antibiotic resistance in a real-world healthcare setting. This type of design is particularly well-suited to analyzing the structural, organizational, and human factors influencing the quality of hospital environmental management at a given time.
Since the dependent variable was dichotomous (high risk of environmental transmission: yes/no), multivariate logistic regression was chosen as the statistical reference method. This approach allows for the estimation of adjusted odds ratios (aORs) while controlling for potential confounding factors, including the existence of an effluent treatment system, the presence of an on-site wastewater treatment plant (WWTP), environmental monitoring, and staff training. The Effluent Management Score (EMS) is based on a multidimensionalconceptualizationofhospitalenvironmental management. This score aggregates several structural and organizational components: effluent treatment, the presence of a wastewater treatment plant, environmental monitoring, management of used antibiotics, and staff training. The scoring approach allows for: • to quantify the overall intensity of environmental management; • to examine the existence of a dose-response effect; • to strengthen the causal plausibility of the association between quality of management and reduction of environmental risk.
The model's performance was evaluated using pseudo-R², n n 1 N + - the Hosmer-Lemeshow test, AUC (ROC curve), sensitivity, and specificity to verify the predictive robustness and internal validity of the results. This analytical strategy ensures consistency between the study objectives, the selected variables, and the interpretation of the results within a One Health perspective that integrates clinical, environmental, and institutional dimensions.
Results
(Management of antibiotic residues in hospital wastewater) Table 1. General characteristics of establishments and practices Variable Dominant modality Estimated proportion (%) Interpretation Type of establishment Clinics / Polyclinics ≥ 60% Strong representation of the private sector Size of establishments < 50 beds ≥ 55% Small to medium capacity structures Existence of a committee for the proper use of antibiotics Yes ≥ 70% Clinical use is relatively regulated. Written prescription protocols Yes ≥ 65% Good level of clinical organization The results in Table 1 show a predominance of private clinics and polyclinics, mostly small to medium-sized (< 50 beds), with a relatively high presence of antibiotic stewardship committees and written prescribing protocols.
This configuration is typical of urban health systems in resource-limited countries, where the private sector plays a central role in healthcare provision but often has limited environmental capacity. Several recent studies confirm that small facilities, although clinically organized, have significant structural deficiencies in hospital wastewater management. Studies have shown that antibiotic prescribing guidelines, when not coupled with adequate environmental management, indirectly contribute to the spread of antibiotic resistance in the environment [15,16]. Omohwovo (2024) specifies that private African facilities prioritize the clinical dimension at the expense of environmental infrastructure [17], by favoring immediate profitability over investments in wastewater treatment [18,19], especially since in low-income countries, policies are often limited to the patient's bedside [19-21].
The pollution load is also directly proportional to the size of the establishment [22]. Furthermore, the diversity of hospital actors without harmonized regulation creates disparate reservoirs of resistance genes (ARG) [23,24]. This is why the existence of committees for the proper use of antibiotics constitutes an important step forward, but remains insufficient in the absence of an integrated One Health approach that includes the environment [25]. Table 2. Management of unused antibiotics and liquid waste. Practical Observed proportion (%) Risk level Disposal of ATB residues at the end of service 50–74% Pupil Disposal after each patient < 25% Moderate No record of quantities disposed of ≥ 60% Pupil Lack of inventory of residues in effluents ≥ 50% Pupil Table 2 highlights high-risk practices, including the uncontrolled disposal of leftover antibiotics at the end of shifts and the lack of traceability records.
These practices facilitate the direct introduction of active molecules into hospital wastewater, creating an environment conducive to the selection of resistant bacteria. Indeed, some authors have demonstrated a direct correlation between the volumes of antibiotics used in hospitals and the concentrations measured in effluents, confirming that the lack of upstream control is a major determinant of pollution [26,27]. It is important to note here that even low concentrations of antibiotics released repeatedly are sufficient to maintain selective pressure in aquatic environments [28,29]. In monitoring, the lack of disposal records prevents any targeted pharmaceutical waste reduction strategy [30,31]. Thus, Hotor et al. (2025), in a meta-analysis in West Africa, identify the poor management of used antibiotics as a central factor in urban water contamination [31].
These data confirm that the practices observed in Lubumbashi constitute a critical link in the environmental transmission chain of resistance. Table 3. Hospital effluent management. Setting Yes (%) No (%) Separation of effluents at the source 50–74% 26–50% Specific treatment of effluents < 25% > 75% Internal wastewater treatment plant (WWTP) 10–24% 76–90% Processing before compliant rejection < 25% ≥ 75% The results in Table 3 show a marked inadequacy of wastewater treatment systems, with less than a quarter of facilities having specific treatment and a low presence of internal wastewater treatment plants. This situation is particularly concerning given the role of hospital wastewater as reservoirs of resistance. This is illustrated by Lymperatou et al.
(2025), who demonstrated that untreated hospital wastewater has high loads of multidrug-resistant bacteria compared to domestic wastewater [33] and that the lack of treatment before discharge is associated with long-term contamination of urban aquatic ecosystems [34]. Cocker et al. (2025) showed the role of urban river networks in sub-Saharan Africa, which act as resistance amplifiers when hospital wastewater is discharged untreated [35]. Based on the above, Fatimazahra et al. (2023) stress that source separation of effluents, although necessary, remains insufficient without secondary or tertiary treatment[36]. Table 4. Environmental monitoring and risk perception. Indicator Proportion (%) Antibiotic residue analyses performed < 10% Reported exceedances of standards ≥ 50% Staff aware of environmental risk ≥ 70% Staff who have received specific training < 25% Table 4 reveals a significant gap between awareness of environmental risk and the effective implementation of antibiotic residue monitoring.
Although over 70% of staff report being aware of the risk, less than 10% of facilities conduct environmental analyses. Yet, Lymperatou et al. (2025) consider the lack of analytical monitoring to be one of the main obstacles to preventing the spread of resistance [33], while Patra et al. (2025) indicate that risk perception, without training or technical tools, does not lead to lasting changes in practices [37], and Endale et al. (2023) and Sambaza and Naicker (2023) emphasize the importance of capacity building to translate awareness into concrete actions [25, 38]. Omohwovo (2024) highlights that the environmental monitoring deficit is a systemic problem in urban Africa [17]. Recent literature highlights that the environmental management of hospital wastewater is a major lever in the fight against antimicrobial resistance.
Studies have shown that the cost of wastewater treatment is significantly lower than the societal costs associated with increased antimicrobial resistance, thus strengthening the economic argument for these investments [39,40]. However, the effective implementation of such strategies depends on appropriate governance mechanisms. Nannini et al. (2022) emphasize the key role of environmental scoring tools in integrating ecological performance into hospital decisionmaking [41]. Furthermore, Dolcini et al. (2025) report strong social acceptability of environmental measures in hospitals, offering a favorable political opportunity [42]. Nevertheless, only the combination of a strengthened regulatory framework and financial incentives can translate this acceptability into sustainable infrastructure [43]. Table 5. Obstacles to the management of antibiotic residues.
Main obstacle Proportion (%) Logistical constraints ≥ 75% Lack of budget ≥ 75% Inadequate training 25–49% Weak regulatory control ≥ 60% The obstacles identified are primarily structural and institutional. Logistical constraints and insufficient budgets, reported by over 75% of facilities, appear to be the major barriers to implementing hospital wastewater treatment systems. Although less frequent (25–49%), inadequate training is an aggravating factor, limiting staff adoption and the sustainability of best practices. Furthermore, the low level of regulatory oversight observed (≥ 60%) reflects insufficient enforcement of existing environmental standards, which significantly reduces the incentive for facilities to invest in sustainable solutions. These results are consistent with those of Hotor et al.
(2025), who identify financial constraints as the main obstacle to the installation of wastewater treatment systems [32]. Similarly, Larsson and Flach (2022) emphasize that the absence of effective environmental regulation reduces institutional commitment to sustainable investments [15]. Finally, Maletic et al. (2025) and Elkoraichi, Y. et al. (2025) confirm that institutional constraints frequently outweigh technical barriers in resource-limited contexts [44, 45]. Table 6. Acceptability of control strategies. Proposed measure Acceptance rate (%) Residue Monitoring Program ≥ 80% Strengthening of effluent treatment ≥ 80% Protocols for managing used antibiotics 60–74% Despite the identified structural constraints, this table reveals a high level of acceptance of the proposed strategies. More than 80% of stakeholders support monitoring antibiotic residues and strengthening effluent treatment, while 60–74% adhere to protocols for managing used antibiotics, reflecting an institutional willingness for change.
These results indicate that the observed obstacles stem more from material, financial, and organizational limitations than from stakeholder refusal. This acceptance constitutes a major lever for targeted and effective interventions, as highlighted by Endale et al. (2023)[25] and Patra et al. (2025)[46]. Table 7. Summary of statistical results relating to the risk of environmental transmission of antibiotic resistance. Dependent variable: High risk of transmission via hospital effluents (Yes = 1; No = 0) A. Bivariate analysis Postman RAW GOLD IC 95% p-value Lack of wastewater treatment 4.52 2.10 – 9.74 < 0.001 Absence of an internal wastewater treatment plant (WWTP) 3.78 1.85 – 7.71 < 0.001 Uncontrolled disposal of antibiotics 3.21 1.42 – 7.23 0.004 Lack of environmental monitoring 4.01 1.92 – 8.36 < 0.001 Staff not trained in effluent management 2.87 1.31 – 6.29 0.008 Bivariate analysis highlights several factors strongly associated with the high risk of environmental transmission of antibiotic resistance via hospital effluents.
The absence of wastewater treatment appears to be the most strongly associated factor, with a probability of risk more than four times higher (crude OR = 4.52; 95% CI: 2.10–9.74; p < 0.001). Similarly, the absence of an on-site wastewater treatment plant (WWTP) is associated with a significant increase in risk (OR = 3.78; 95% CI: 1.85–7.71). Uncontrolled antibiotic disposal is also significantly associated with high risk (OR = 3.21), highlighting the importance of upstream management practices. The absence of environmental monitoring has a comparable effect (OR = 4.01), reflecting the critical role of effluent monitoring in preventing the spread of resistant strains. Finally, lack of staff training is associated with a risk almost three times higher (OR = 2.87), indicating that human factors contribute substantially to environmental risk.
B. Multivariate logistic regression Variable Adjusted OR (aOR) IC 95% p-value Effluent management score (per point) 0.62 0.48 – 0.79 < 0.001 Good management (SGE 4–5) vs. poor (0–2) 0.18 0.07 – 0.41 < 0.001 Moderate management (SGE = 3) vs. low 0.45 0.22 – 0.89 0.021 Lack of wastewater treatment 3.92 1.88 – 8.17 < 0.001 No STEP 3.21 1.54 – 6.68 0.002 Lack of environmental monitoring 3.67 1.72 – 7.84 < 0.001 Untrained staff 2.41 1.16 – 5.03 0.018 After adjusting for confounding factors, multivariate logistic regression confirms that hospital effluent management is a major independent determinant of the risk of environmental transmission. The Effluent Management Score (EMS) showed a significant protective effect, with each one-point increase associated with a 38% reduction in risk (aOR = 0.62; 95% CI: 0.48–0.79; p < 0.001).
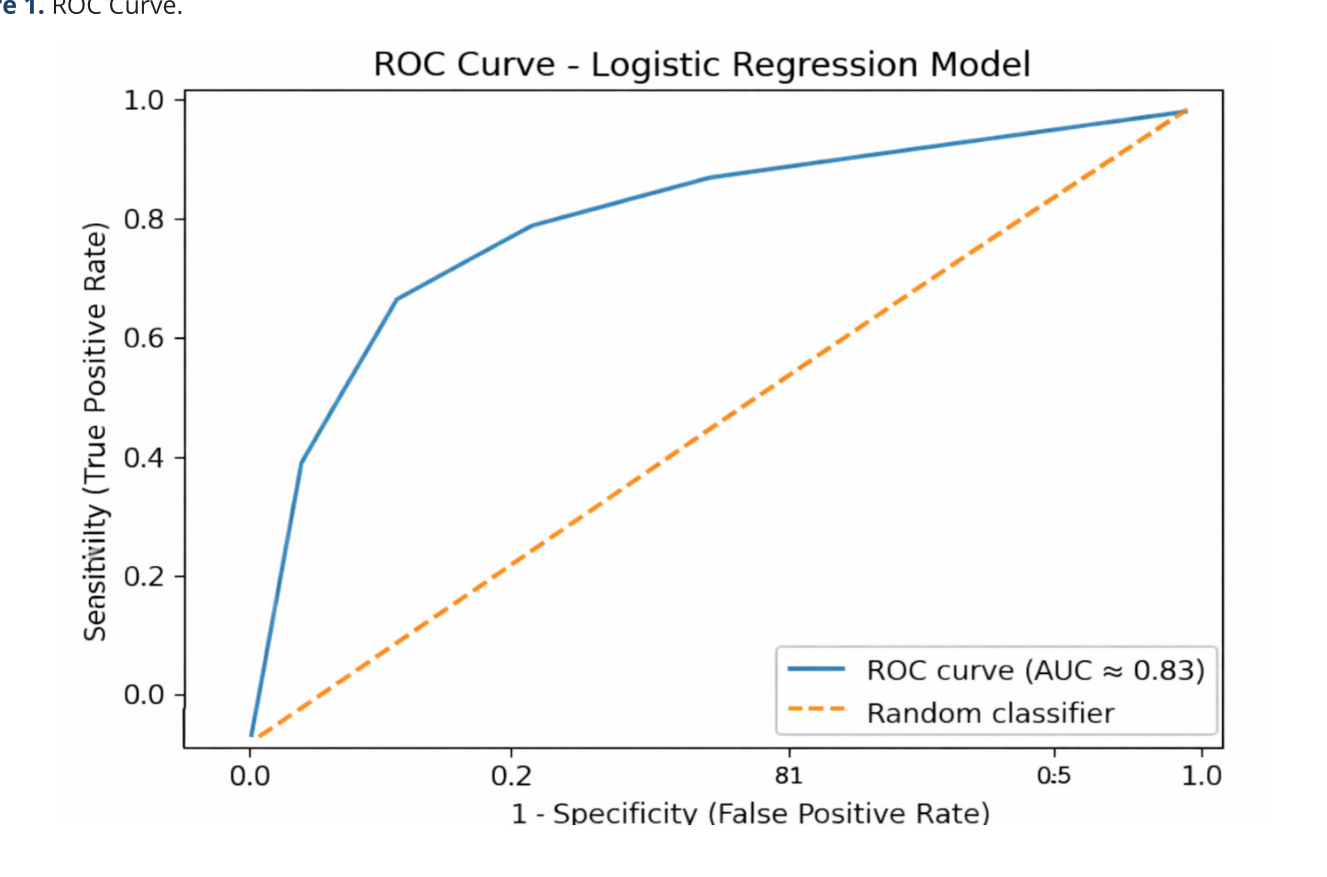
This dose-response relationship strengthens the hypothesis of a causal link between the quality of effluent management and risk reduction. Facilities with good effluent management (SGE 4–5) have a reduced risk of approximately 82% compared to those with poor management (aOR = 0.18), while moderate management also confers a significant protective effect. Moreover, even after adjustment, the lack of effluent treatment, the absence of wastewater treatment plants, the lack of environmental monitoring and the lack of staff training remain significantly associated with high risk, with adjusted odds ratios greater than 2, confirming their independent role. C. Model Quality and Performance Indicator Value -2 Log Likelihood 118.6 Pseudo-R² (Cox & Snell) 0.29 Pseudo-R² (Nagelkerke) 0.41 Hosmer–Lemeshow test (χ²; p-value) 6.84; 0.55 AIC 134.6 BIC 158.2 Sensitivity 81.3% Specificity 76.5% Correct classification rate 79.1% AUC (ROC) 0.83 (95% CI: 0.75–0.90) Statistical indicators show that the model used is reliable and relevant.
Nagelkerke's pseudo-R² (0.41) means that the model explains a significant portion of the phenomenon studied, which is considered high in observational public health studies. The Hosmer-Lemeshow test (p = 0.55) indicates that the model fits the observed data well; in other words, the predicted results correspond well to reality. The model's ability to correctly identify risky situations is also good: it detects more than 8 out of 10 cases (sensitivity 81.3%), while correctly identifying nearly 3 out of 4 risk-free cases (specificity 76.5%). The area under the ROC curve (AUC = 0.83) confirms an excellent ability to distinguish between high- and low-risk situations. Multivariate analysis clearly shows that the quality of hospital effluent management plays a decisive and independent role in reducing the risk of resistance dissemination.
The higher the Effluent Management Score, the lower the risk, reflecting a robust dose-response relationship. Similar results were reported by Deedat and Lymperatou (2025), who showed that a progressive improvement in environmental practices significantly reduces the resistance load in effluents [33, 26]. Conversely, Cocker et al. (2025) confirm that the absence of treatment and monitoring increases the risk of dissemination [35]. Receiver Operating Characteristic (ROC) curve of the multivariate logistic regression model assessing the high risk of environmental transmission of antibiotic resistance via hospital effluents in Lubumbashi (DRC). The area under the curve (AUC) was 0.83 (95% CI: 0.75–0.90; p < 0.001), indicating excellent discriminatory power of the model. Figure 1.
ROC Curve. The ROC curve allows us to appreciate the ability of the logistic regression model to correctly differentiate establishments exposed to a high risk of environmental dissemination of antibiotic resistance from those with a low risk. In this study, an area under the curve (AUC) of 0.83 (95% CI: 0.75–0.90) indicates a high discriminatory capacity. In other words, the model has an 83% probability of assigning a higher risk level to a truly high-risk institution compared to a nonexposed institution. Furthermore, the sensitivity (81.3%) / specificity (76.5%) ratio reflects a satisfactory balance between detecting atrisk situations and limiting misclassification errors. The nonsignificant Hosmer–Lemeshow test (p = 0.55) confirms a good overall fit of the model, indicating a good match between the estimated probabilities and the observed data.
All of these indicators support the validity of the model as a decisionmaking tool in hospital environmental health. The observed performance is consistent with the results reported in recent literature on hospital effluent monitoring. The narrative review by Diamantina Lymperatou et al. (2025) highlights that models combining structural indicators (presence of treatment, internal treatment plants) and organizational indicators (environmental monitoring, staff training) generally have AUCs between 0.75 and 0.85, values comparable to those obtained in the present study [33]. In a consistent manner, the pilot study by Fatima Deedat et al. (2025) demonstrates that the integration of data relating to hospital use of antibiotics and residual concentrations measured in effluents allows for reliable discrimination of environmental risk, with AUCs greater than 0.80 [36].
In an African context, the work of David Cocker et al. (2025) shows that the absence of treatment and monitoring devices for effluents significantly increases the contamination of urban river networks, highlighting the strategic importance of effectivepredictivemodelstoguidetargetedinterventions[35]. Finally, the meta-analysis conducted by Paul Hotor et al. (2025) confirms that untreated hospital effluents constitute major reservoirs of resistance genes, and explicitly recommends the use of statistical tools with high discriminatory power to prioritize investment in resource-limited countries [32]. Thus, an AUC of 0.83 not only reflects good statistical performance but also demonstrates the model's real operational utility for guiding hospital policies in Lubumbashi. It reliably identifies facilities where improved wastewater management (treatment, wastewater treatment plants, environmental monitoring, and staff training) could generate the most immediate benefits in terms of reducing the environmental risk associated with antimicrobial resistance.
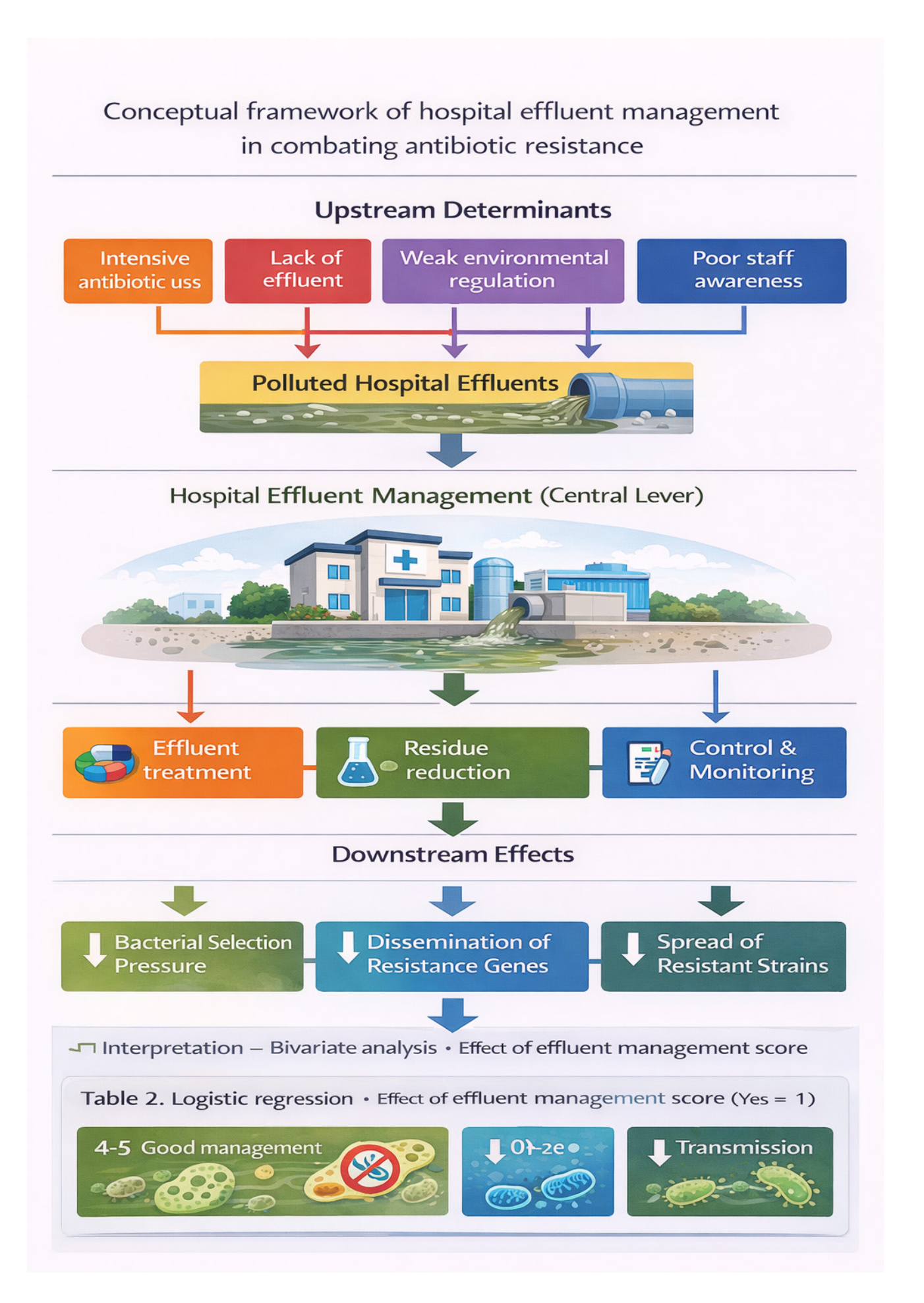
To structure the analysis and illustrate the theoretical and empirical relationships between the different variables studied, a conceptual framework was developed. This framework is based on the hypothesis that hospital wastewater management is a key environmental factor in the transmission of antibiotic-resistant bacterial strains. This framework brings together the main structural, organizational and human factors — such as effluent treatment, the existence of internal treatment plants, environmental monitoring, management of used antibiotics and staff training — that influence the presence of antibiotic residues and resistance genes in effluents, and consequently the risk of environmental dissemination. It also incorporates the moderating effect of financial, logistical, and regulatory constraints within a One Health approach that integrates clinical, environmental, and institutional dimensions.
This framework forms the analytical basis for interpreting the results, developing the Effluent Management Score, and formulating recommendations tailored to the Lubumbashi hospital context.
Conclusion
This study highlights that inadequate management of hospital wastewater is a major environmental determinant of the spread of antibiotic resistance in Lubumbashi. Despite the existence of antibiotic stewardship programs, the results show that the lack of wastewater treatment, insufficient environmental monitoring, and inadequate staff training are significantly associated with a high risk of environmental transmission of resistant strains. Multivariate logistic regression confirms that integrated and structured wastewater management, as measured by the Wastewater Management Score, has a significant protective effect, with risk reductions exceeding 80% in the best-equipped facilities. These results underscore that the fight against antibiotic resistance must extend beyond the clinical setting to fully integrate the environmental dimension.
The progressive improvement of hospital wastewater management thus represents a strategic, realistic, and essential lever in resourcelimited settings, in line with the One Health approach. Recommendations 1. Institutional and regulatory recommendations • To establish and make operational hospital effluent treatment systems adapted to the local context; • Strengthen the application of environmental standards relating to hospital discharges; • Integrate antibiotic residue management into national and provincial policies to combat antibiotic resistance 2. Technical and environmental recommendations • Install wastewater treatment plants (primary or secondary) in hospital facilities; • Ensure the effective reduction of antibiotic residues before release into the environment; • Implement regular monitoring of hospital effluents to detect antibiotic residues and indicators of resistance.
3. Recommendations related to human resources • Train hospital and technical staff on liquid waste management and the environmental impact of antibiotics ; • Appoint environmental management officers within healthcare facilities; • Strengthen collaboration between clinicians, pharmacists, biologists and environmental managers. 4. Recommendations in public health and research • Adopt an integrated One Health approach combining human health, environment and governance; • Raising awareness among decision-makers and the community about the risks associated with antibiotic residues in the environment; • Encourage operational research on environmental monitoring of antibiotic resistance. The fight against antibiotic resistance is not limited to the clinical use of antibiotics; it also involves controlling their environmental impact.
Effective management of hospital wastewater is a sustainable and essential strategy for preventing the transmission of resistant strains.
Figures and Tables
References
- Larsson DGJ, Flach CF. Antibiotic resistance in the environment. Nat Rev Microbiol. 2022 May;20(5):257- 269. doi:10.1038/s41579-021-00649-x Epub 2021 Nov 4. PMID: 34737424; PMCID: PMC8567979.
- Endale H, Mathewos M, Abdeta D. Potential Causes of Spread of Antimicrobial Resistance and Preventive Measures in One Health Perspective-A Review. Infect DrugResist.2023;16:7515-7545https://doi.org/10.2147/ IDR.S428837
- Patra M, Gupta AK, Kumar D, Kumar B. Antimicrobial Resistance: A Rising Global Threat to Public Health. Infect Drug Resist. 2025 Oct 23;18:5419-5437. doi: 10.2147/ IDR.S530557. PMID: 41158783; PMCID: PMC12558087.
- Deedat FZ, Faya AM, Gumbi BP, Johnston DMG, Karpoormath R, Essack SY. The association between antibiotic use in hospitals and residual antibiotic concentrations in hospital effluents: a pilot study. JAC Antimicrob Resist. 2025 May 12;7(3):dlaf070. doi:10.1093/jacamr/dlaf070 PMID: 40356741; PMCID: PMC12066823.
- Md Ariful Haque, Lindsay Rogerson, Nirmalendu Deb Nath, Samuel Haruna, Jaehyun Ahn, Tony V. Johnston, Carol Sze Ki Lin, Li Chong, Li Na, Min Ji Jang, Seockmo Ku,Sustainable management and valorization of antibiotic waste,Chemical Engineering Journal,Volume 498,2024,155372,ISSN1385-8947,https://doi org/10.1016/j.cej.2024.155372
- Hotor P, Kotey FCN, Donkor ES. Antibiotic resistance in hospital wastewater in West Africa: a systematic review and meta-analysis. BMC Public Health. 2025 Apr 11;25(1):1364. doi:10.1186/s12889-025-22513-w PMID: 40217451; PMCID: PMC11987346.
- Kasamba Ilunga Eric. et al. “Wastewater, A Reservoir of Antibiotic-Resistant Bacteria” International Journal of Research Studies in Microbiology and Biotechnology (IJRSMB), vol 10, no. 1, 2025, pp. 1-9.DOI: https://doi org/10.20431/2454-9428.01001001
- Omohwovo EJ. Wastewater Management in Africa: Challenges and Recommendations. About Health Insights. 2024 Oct 9;18:11786302241289681. doi:10.1177/11786302241289681 PMID: 39399328; PMCID: PMC11467993.
- Cocker, D., Mwapasa, T., Grabic, R. et al. Environmental hazards from pollution of antibiotics and resistancedriving chemicals in an urban river network from Malawi. npj Antimicrob Resist 3, 85 (2025). https://doi org/10.1038/s44259-025-00149-5
- Lymperatou D, Konstantopoulou R, Mentsis M, AtzemoglouN,DiamantiC,TzourtzosI,NakaKK,MitsisM, Konstantina G, Milionis H, Ntzani E, Christaki E. Hospital Wastewater Surveillance and Antimicrobial Resistance: A Narrative Review. Microorganisms. 2025 Nov 30;13(12):2739. doi: 10.3390/microorganisms13122739 PMID: 41471943; PMCID: PMC12735555.
- Manuela Macrì, Sara Bonetta, Andrea Di Cesare, Raffaella Sabatino, Gianluca Corno, Marta Catozzo, Cristina Pignata, Enrica Mecarelli, Claudio Medana, Elisabetta Carraro, Silvia Bonetta,Antibiotic resistance and pathogen spreading in a wastewater treatment plant designed for wastewater reuse,Environmental Pollution,Volume 363, Part 1,2024,125051,ISSN 0269- 7491, https://doi.org/10.1016/j.envpol.2024.125051
- Shepherd Sundayi Sambaza, Nisha Naicker,Contribution of wastewater to antimicrobial resistance: A review article,JournalofGlobalAntimicrobialResistance,Volume 34,2023,Pages 23-29,ISSN 2213-7165, https://doi org/10.1016/j.jgar.2023.05.010
- Aguilar-Rangel EJ, Paredes-Cárcamo F, Andrade MD, Contreras-Sánchez D, Rain-Medina V, Campanini- Salinas J, Medina DA. Hospital Wastewater as a Reservoir of Contaminants of Emerging Concern: A Study Report from South America, Chile. Antibiotics (Basel). 2025 Nov 4;14(11):1111. doi: 10.3390/antibiotics14111111 PMID: 41301606; PMCID: PMC12649306.
- Fatimazahra S, Latifa M, Laila S, Monsif K. Review of hospital effluents: special emphasis on characterization, impact, and treatment of pollutants and antibiotic resistance. About Monit Assess. 2023 Feb 13;195(3):393. doi:10.1007/s10661-023-11002-5 PMID: 36780024; PMCID: PMC9923651.
- Larsson, DGJ, Flach, CF. Antibiotic resistance in the environment. Nat Rev Microbiol 20, 257–269 (2022). https://doi.org/10.1038/s41579-021-00649-x 16. Ågerstrand, M., Josefsson, H., Wernersson, AS. et al. Opportunities to tackle antibiotic resistance development in the aquatic environment through the Water Framework Directive. Ambio 52, 941–951 (2023). https://doi.org/10.1007/s13280-022-01828-7
- Omohwovo EJ. Wastewater Management in Africa: Challenges and Recommendations. About Health Insights. 2024 Oct 9;18:11786302241289681. doi:10.1177/11786302241289681 PMID: 39399328; PMCID: PMC11467993.
- Mohammad Ramezanianpour, Victoria Fryer, Akbar Ali, Wenzhi Xu, Mehdi Shayegh,Hierarchical prioritization of on-site wastewater treatment systems using combined decision analysis and Microsoft Visual Basic,Journal of WaterProcessEngineering,Volume55,2023,104135,ISSN 22147144, https://doi.org/10.1016/j.jwpe.2023.104135
- JoseCarlosAsfor,NeurisangeloCavalcantedeFreitasand Placido Rogério Pinheiro.Prioritization of Investments in Sewage Projects: A Multicriteria Model. Water 2025, 17(21), 3065;https://doi.org/10.3390/w17213065
- Saleem Z, Mekonnen BA, Orubu ES, Islam MA, Nguyen TTP, Ubaka CM, Buma D, Thuy NDT, Sant Y, Sono TM, Bochenek T, Kalungia AC, Abdullah S, Miljković N, Yeika E, Niba LL, Akafity G, Sefah IA, Opanga SA, Kitutu FE, Khuluza F, Zaranyika T, Parajuli A, Darweesh O, Islam S, Kumar S, Nabayiga H, Jairoun AA, Chigome A, Ogunleye O, Fadare J, Massele A, Cook A, Jelić AG, Godói IPD, Phillip A, Meyer JC, Funiciello E, Lorenzetti G, Kurdi A, Haseeb A, Moore CE, Campbell SM, Godman B, Sharland M. Current access, availability and use of antibiotics in primary care among key low- and middle-income countries and the policy implications. Expert Rev Anti Infect Ther. 2025 Apr 15:1-42. doi:10.1080/14787210.2 025.2477198. Epub ahead of print. PMID: 40110804.
- Kanan M, Ramadan M, Haif H, Abdullah B, Mubarak J, Ahmad W, Mari S, Hassan S, Eid R, Hasan M, Qahl M, Assiri A, Sultan M, Alrumaih F, Alenzi A. RETRACTED: Empowering Low- and Middle-Income Countries to Combat AMR by Minimal Use of Antibiotics: A Way Forward. Antibiotics (Basel). 2023 Oct 2;12(10):1504. Antibiotics (Basel). 2025 Jan 14;14(1):84. doi: 10.3390/ antibiotics14010084. PMID: 37887205; PMCID: PMC10604829.
- Parida VK, Sikarwar D, Majumder A, Gupta AK. An assessment of hospital wastewater and biomedical waste generation, existing legislations, risk assessment, treatment processes, and scenario during COVID-19. J Environ Manage. 2022 Apr 15;308:114609. doi: 10.1016/j.jenvman.2022.114609 Epub 2022 Jan 26. PMID: 35101807; PMCID: PMC8789570.
- Lan L, Wang Y, Chen Y, Wang T, Zhang J, Tan B. A Review on the Prevalence and Treatment of Antibiotic Resistance Genes in Hospital Wastewater. Toxics. 2025 Mar 31;13(4):263. doi:10.3390/toxics13040263 PMID: 40278579; PMCID: PMC12031161.
- Ikhwan Yuda Kusuma, Hening Pratiwi, Afriza Pujiati, Septi Nurkhasanah, Dian Ayu Eka Pitaloka,Antibiotic Residues, Resistant Bacteria, and Resistance Genes in Hospital Wastewater from Upper Middle-Income Countries: A Systematic Review,Current Opinion in Environmental Science & Health,2026,100707,ISSN 2468-5844, https:// doi.org/10.1016/j.coesh.2026.100707
- Endale H, Mathewos M, Abdeta D. Potential Causes of Spread of Antimicrobial Resistance and Preventive Measures in One Health Perspective-A Review. Infect Drug Resist. 2023 Dec 8;16:7515-7545. doi: 10.2147/IDR S428837. PMID: 38089962; PMCID: PMC10715026.
- Deedat FZ, Faya AM, Gumbi BP, Johnston DMG, Karpoormath R, Essack SY. The association between antibiotic use in hospitals and residual antibiotic concentrations in hospital effluents: a pilot study. JAC Antimicrob Resist. 2025 May 12;7(3):dlaf070. doi:10.1093/jacamr/dlaf070 PMID: 40356741; PMCID: PMC12066823.
- Coulibaly B, Pastor-López EJ, Diawara A, Savane FB, Escolà-Casas M, Matamoros V, Ba S. Occurrence of antibiotics in hospital wastewater effluents discharged into the Niger River in Bamako, Mali. Risk assessment and solutions. About Pollut. 2025 Apr 15;371:125912. PMID: 40010595.
- Donkor ES, Odoom A, Hotor P. Antibiotic Concentrations in Aquatic Environments of the African Continent: A Systematic Review and Predicted No-Effect Concentration (PNEC) Assessment. About Health Insights. 2025 Nov 17;19:11786302251391299. doi:10.1177/11786302251391299 PMID: 41262987; PMCID: PMC12623662.
- Ileana Federigi, Silvia Bonetta, Marina Tesauro, Osvalda De Giglio, Gea Oliveri Conti, Nebiyu Tariku Atomsa, Francesco Bagordo, Sara Bonetta, Michela Consonni, Giusy Diella, Margherita Ferrante, Alfina Grasso, Manuela Macrì, Maria Teresa Montagna, Marco Verani, Annalaura Carducci,A systematic scoping review of antibiotic-resistance in drinking tap water,Environmental Research,Volume 263, Part 1,2024,120075,ISSN 0013-9351,https://doi org/10.1016/j.envres.2024.120075
- Kumar, A., Thakur, AK, Gaurav, GK et al. A critical review on sustainable hazardous waste management strategies: a step towards a circular economy. Environ Sci Pollut Res 30, 105030–105055 (2023). https://doi org/10.1007/s11356-023-29511-8
- Haneen Alrabiah, Vian Ahmed, Zied Bahroun,A systematic review of waste management practices in the healthcare sector,Cleaner Waste Systems,Volume 12,2025,100400,ISSN 2772-9125,https://doi org/10.1016/j.clwas.2025.100400
- Hotor, P., Kotey, FCN & Donkor, ES Antibiotic resistance in hospital wastewater in West Africa: a systematic review and meta-analysis. BMC Public Health 25, 1364 (2025). https://doi.org/10.1186/s12889-025-22513-w
- Diamantina Lymperatou,Revekka,Konstantopoulou,- Michalis Mentsi,Natalia Atzemoglou1,Christina Diamanti,Ioannis Tzourtzos,Katerina K. Naka,Michail Mitsis,Gartzonika Konstantina,Eirini Christaki1,Hospital Wastewater Surveillance and Antimicrobial Resistance: A Narrative Review; Microorganisms 2025, 13(12), 2739;https://doi.org/10.3390/microorganisms13122739
- Eduardo J. Aguilar-Range,Francisca Paredes- Cárcamo,Maikol D. Andrade,Danilo Contreras- Sánchez3,4Vanessa Rain-Medina,Javier Campanini- Salinas,and Daniel A. Medina.Hospital Wastewater as a Reservoir of Contaminants of Emerging Concern: A Study Report from South America, Chile. Antibiotics2025, 14(11), 1111; https://doi.org/10.3390/ antibiotics14111111
- Cocker D, Mwapasa T, Grabic R, Grabicová K, Staňová AV, Chidziwisano K, Roberts AP, Morse T, Feasey NA, Singer AC. Environmental hazards from pollution of antibiotics and resistance-driving chemicals in an urban river network from Malawi. NPJ Antimicrob Resist. 2025 Oct 9;3(1):85. doi:10.1038/s44259-025-00149-5 PMID: 41068296; PMCID: PMC12511589.
- Fatimazahra S, Latifa M, Laila S, Monsif K. Review of hospital effluents: special emphasis on characterization, impact, and treatment of pollutants and antibiotic resistance. About Monit Assess. 2023 Feb 13;195(3):393. doi:10.1007/s10661-023-11002-5 PMID: 36780024; PMCID: PMC9923651.
- Petropoulos, F., Akkermans, H., Aksin, OZ, Ali, I., Babai, MZ, Barbosa-Povoa, A., … Zheng, T. (2026). Operations & supply chain management: principles and practice. International Journal of Production Research, 64(1), 330– 513. https://doi.org/10.1080/00207543.2025.255553
- Sambaza SS, Naicker N. Contribution of wastewater to antimicrobial resistance: A review article. J Glob Antimicrob Resist. 2023 Sep;34:23-29. doi: 10.1016/j jgar.2023.05.010. Epub 2023 Jun 5. PMID: 37285914.
- Lihua Lan,Yixin Wang,Yuxin Chen,Ting Wang,Jin Zhang,Biqin Tan. A Review on the Prevalence and Treatment of Antibiotic Resistance Genes in Hospital Wastewater. Toxics 2025, 13(4), 263; https://doi org/10.3390/toxics1304026
- Nuhu Amin, Tim Foster, Nafeya Tabassum Shimki, Juliet Willetts,Hospital wastewater (HWW) treatment in low- and middle-income countries: A systematic review of microbial treatment efficacy,Science of The Total Environment,Volume 921,2024,170994,ISSN 0048-9697, https://doi.org/10.1016/j.scitotenv.2024.170994
- Nannini M, Biggeri M, Putoto G. Health coverage and financial protection in Uganda: a political economy perspective. Int J Health Policy Manag. 2022;11(9):1894– 1904. doi:10.34172/ijhpm.2021.116
- Dolcini M, Ferrè F, Brambilla A, Capolongo S. Integrating environmental sustainability into hospitals performance management systems: a scoping review. BMC Health Serv Res. 2025 May 28;25(1):764. doi:10.1186/s12913- 025-12928-x. PMID: 40437479; PMCID: PMC12117838.
- Masood Ahmed, Eduardo Araral, Muhammad Asif Khan,Barriers to just energy transition: Institutional and infrastructure challenges in developing countries,- Sustainable Futures,Volume 10,2025,101414,ISSN2666- 1888,https://doi.org/10.1016/j.sftr.2025.101414 (https://www.sciencedirect.com/science/article/pii/ S266618882500975X )
- Maletič D, Trojanowska J, Lorber M, Maletič M. Identification and prioritization of barriers to the implementation of an asset management system in the healthcare sector using a Delphi-AHP approach. J Health Organ Management. 2025 Dec 15;39(9):535–60. PMCID: PMC12686151.
- Elkoraichi, Y., Elfezazi, S. & Belhadi, A. Analysis of barriers to blockchain technology adoption in the African agrifood supply chain. Discov Sustain 6, 289 (2025). https:// doi.org/10.1007/s43621-025-01125-9
- Patra M, Gupta AK, Kumar D, Kumar B. Antimicrobial Resistance: A Rising Global Threat to Public Health. Infect Drug Resist. 2025 Oct 23;18:5419-5437. doi: 10.2147/ IDR.S530557. PMID: 41158783; PMCID: PMC12558087
This is a text version generated from the article. For the formatted version of record (with original tables & figures), download the PDF →