Full Text Hide / show
Background
: Central retinal artery occlusion (CRAO) is an ophthalmic emergency most commonly related to carotid atherosclerosis or cardiac embolism in younger patients. Calcific aortic valve disease is an uncommon source of retinal emboli and rarely presents first as CRAO. Case Presentation: A 30-year-old man with a 7.5 pack-year smoking history presented with sudden, painless, complete left monocular vision loss. Ophthalmic assessment including fundus exam and fluorescein angiography confirmed left central retinal artery occlusion with preserved cilioretinal artery perfusion. Two weeks earlier he had transient chest pain. Cardiac examination revealed a harsh grade III/IV systolic ejection murmur radiating to the carotids. ECG showed sinus rhythm with LV hypertrophy and anterior ST elevation.
Transthoracic echocardiography demonstrated moderate–severe aortic stenosis (mean gradient ~40 mmHg), markedly calcified valve with poorly visualized cusps, concentric LV hypertrophy and preserved LVEF (60%). CT chest showed ascending aortic dilation (4.3 cm). Coronary angiography revealed ostial right coronary artery stenosis; cerebral CT and brain MRI/MRA showed no intracranial arterial occlusion. The patient underwent urgent surgical aortic valve replacement; intraoperative inspection revealed a severely stenotic bicuspid aortic valve with large friable calcific vegetations at the fused raphe. A mechanical prosthesis was implanted without complication. Postoperative recovery was uneventful; no further systemic embolic events occurred. Visual prognosis remained limited. Discussion: This case highlights an unusual presentation of calcific bicuspid aortic valve disease in a young adult, manifesting as CRAO.
Retinal calcium microemboli may be clinically apparent due to the retina’s end-arterial circulation. Identification of a cardiac source—particularly heavily calcified aortic valve—is critical because embolic events may recur and can be bilateral. Urgent cardiac evaluation and consideration of valve replacement are warranted even when conventional hemodynamic indications are borderline, given the embolic risk. Conclusion: CRAO can be the initial manifestation of calcific aortic stenosis. In young patients with retinal artery occlusion, prompt cardiac assessment for valvular calcification (including echocardiography and, where indicated, catheterization) should be undertaken. Urgent valve replacement should be considered to prevent recurrent systemic embolization. Keywords: Central retinal artery occlusion; retinal embolus; calcific aortic stenosis; bicuspid aortic valve; valve replacement; calcium embolus.
Introduction
- Brief overview of CRAO, standard etiologies (carotid atherosclerosis, cardiac sources), urgency of diagnosis and limited retinal ischemia time. - Note rarity of calcific aortic valve disease presenting as retinal embolization, particularly in younger patients.
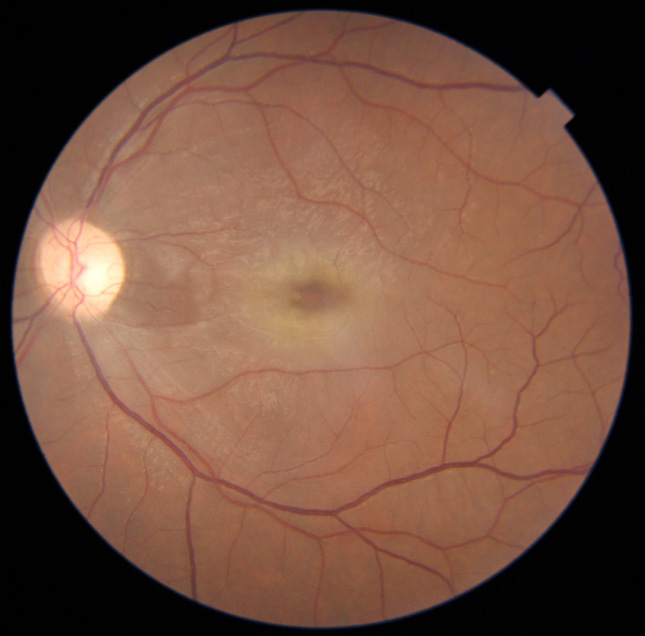
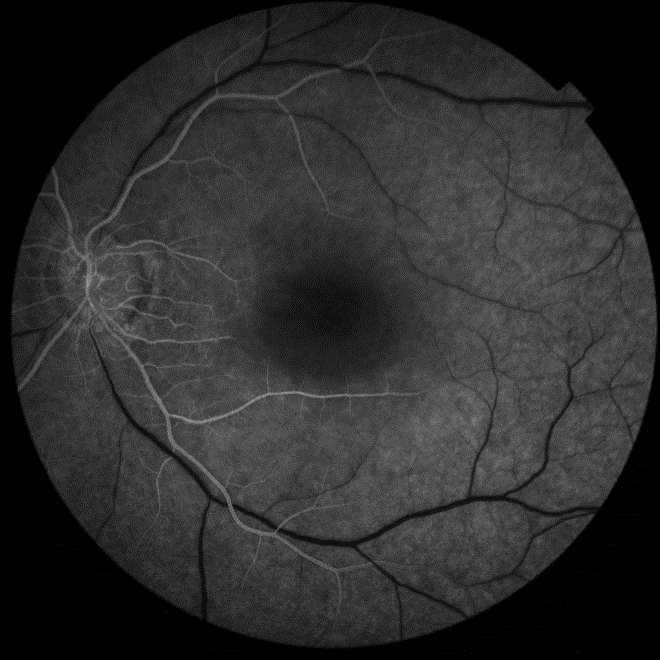
Case Presentation - Patient demographics: 30-year-old male, smoker (7.5 pack-years), prior alcohol use, otherwise healthy. - Presenting complaint: sudden, painless loss of vision in the left eye. - Relevant history: transient chest pain 2 weeks prior; family history notable for bicuspid aortic valve and coarctation in father. - Examination: left monocular vision loss with afferent pupillary defect, normal extraocular movements and anterior segment exam; grade III/IV harsh systolic ejection murmur at RUSB with carotid radiation. Investigations - Ophthalmology: Dilated fundus exam — pale retina with cherry-red spot; possible visible arteriolar embolus. Fluorescein angiography — absence of retinal arterial filling except cilioretinal artery; delayed venous filling. - ECG: sinus rhythm, LV hypertrophy, ST elevation V1–V4.
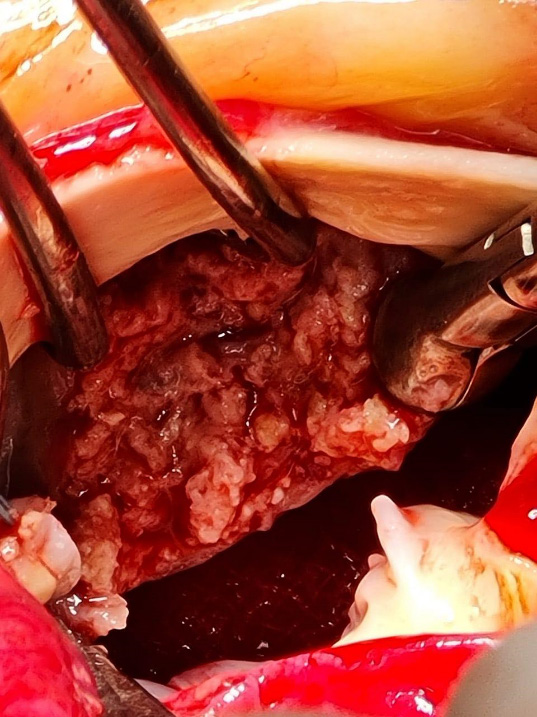
- Transthoracic echocardiogram: moderate–severe aortic stenosis (mean gradient ≈40 mmHg), markedly calcified valve with probable bicuspid morphology, concentric LV hypertrophy (wall thickness 1.9 cm), LVEF 60%, normal aortic root (3.5 cm). - CT chest: ascending aorta dilation 4.3 cm. - Coronary angiography: ostial right coronary artery stenosis; otherwise normal coronaries. - Brain CT/MRI/MRA: no intracranial arterial stenosis or aneurysm; supra-aortic carotids normal. *** Treatment - Multidisciplinary decision for urgent surgical aortic valve replacement due to risk of recurrent embolization from friable calcific valve. - Intraoperative findings: severely stenotic bicuspid aortic valve with large, friable calcific vegetations at fused raphe between left and right cusps. - Procedure: mechanical aortic valve implantation; no intraoperative complications.
**Outcome and Follow-up - Uneventful postoperative recovery; no further embolic events. - Ophthalmic prognosis: persistent visual loss in affected eye consistent with CRAO; cilioretinal-sparing limited central vision. - Cardiac follow-up: routine postoperative surveillance and anticoagulation per mechanical valve protocol.
Discussion
- Emphasize rarity of CRAO as initial manifestation of calcific aortic valve disease, particularly in a young adult. - Pathophysiology: calcium microemboli from a heavily calcified, friable valve travel to retinal circulation; unique vulnerability of retinal end-arterial circulation leads to overt visual loss even when emboli would be clinically silent elsewhere. - Diagnostic approach: in CRAO—urgent ophthalmic investigations plus systemic embolic workup including carotid imaging and cardiac evaluation (echo ± TEE, CT/ CATH as indicated). In young patients or when embolic material appears calcific (white), consider aortic valve calcification as a source. - Management implications: While valve replacement is typically guided by hemodynamics and symptoms, embolic events from valvular calcification represent a valid indication for prompt surgical intervention to prevent recurrent, potentially bilateral embolization.
- Literature context: summarize briefly that reported cases are few; existing reports support valve surgery in similar settings. - Limitations: single case; visual outcome limited due to delayed retinal reperfusion window.
Conclusion
CRAO can be the presenting manifestation of calcific bicuspid aortic valve disease. Prompt cardiac evaluation and consideration of urgent valve replacement are warranted to prevent recurrent embolic events, even when classical surgical indications are marginal. Figure 1. Fundus photograph — pale retina with cherry-red spot (left eye). Figure 2. Fundus showing segmented/narrowed arterioles and visible embolus (if present). Figure 3. Fundus showing segmented/narrowed arterioles and visible embolus (if present). Figure 4. Fluorescein angiogram — early phase showing absent retinal arterial filling except cilioretinal artery; delayed venous filling.
Figures and Tables

References
- Hayreh SS. Central retinal artery occlusion. Indian J Ophthalmol. 2018;66(12):1684–1695. doi:10.4103/ijo IJO_1861_18
- Biousse V, Calvetti O, Newman NJ. Retinal artery occlusion: acute management and treatment. Curr Opin Ophthalmol. 1998;9(6):45–54.
- Chang HM, Lee T, Park SJ, et al. Calcific aortic valve disease and systemic embolization: case reports and review. Clin Cardiol. 1996;19(3):219–224. doi:10.1002/ clc.4960190322
- Brown GC, Magargal LE. Central retinal artery occlusion: visual outcome after treatment. Am J Ophthalmol. 1981;92(4):541–547.
- Hayreh SS, Zimmerman MB. Central retinal artery occlusion: visual outcome. Am J Ophthalmol. 2006;142(6):986–987. doi:10.1016/j.ajo.2006.07.015
This is a text version generated from the article. For the formatted version of record (with original tables & figures), download the PDF →