Full Text Hide / show
Introduction
The American Journal of Public Health Novel Binary Drugs Against Respiratory Viruses: Combined Virus- And Host-Targeted Approach. Health. 2026 June; 17(1). doi: 10.52338/tajoph.2026.5816. use, Minireview O.P. Zhirnov 1, 2) (1)D.I. Ivanovsky Institute of Virology, N. F. Gamaleya Scientific Research Institute of Epidemiology and Microbiology, Moscow 123098, Russia Email: [email protected]. (2)The Russian-German Academy of Medicosocial and Biotechnological Sciences, Moscow 121205, Skolkovo, Moscow Innovation Center, Russia. Abstract Influenza and coronaviruses are relevant respiratory infections that cause significant damage to people’s health and healthcare systems. Modern antiviral drugs with direct viral action (VTA – virus-targeting action) have several disadvantages related to (i) a narrow spectrum of antiviral action, (ii) the rapid appearance of drug-resistant mutants, (iii) a lack of drug action to suppress the pathogenesis of viral diseases, and (iv) high therapeutic dosages and side effects.
This minireview focuses on the design of drugs that target both viral (VTA) and cellular pathogenetic mechanisms (HTA – host-targeting action). This type of binary drug is designed to overcome the above limitations of the monotarget approach. An effective binary drug combining aprotinin, a natural polypeptide protease inhibitor, and ribavirin, a nucleoside analogue interfering with viral polymerase, is considered. Aerosol inhalations of this combined formulation were found to prevent virus dissemination and develop high therapeutic efficacy in mice infected with the highly pathogenic H7N2 avian influenza virus. This type of pharmaceutical formulation is applicable for aerosol delivery using a propellant metered-dose inhaler in patients at the earliest signs of respiratory infection.
Thus, binary antiviral drugs open a promising avenue for creating reliable drugs to combat new, unknown viral threats of future highly pathogenic viral diseases “X”. Keywords: respiratory infections, viruses, antivirals, disease “X”, aprotinin, ribavirin, inhalers, host-targeted, virus-targeted, drugs. ACTUALITY OF RESPIRATORY VIRUS INFECTIONS Respiratory viral infections continue to be a leading cause of acute illness, contributing to the global healthcare burden, particularly for infants, the elderly and immunocompromised individuals. Among these infections, the most prevalent are those caused by influenza viruses, coronaviruses, respiratory syncytial virus, human rhinoviruses, and human paramyxoviruses. Over the last decade, lower respiratory tract infections have caused 2–3 million deaths worldwide annually [1]. Additionally, there is a potential medical threat: the emergence of novel, unknown, and dangerous pathogens, such as highly pathogenic avian influenza viruses, severe acute respiratory syndrome coronaviruses, monkeypox virus, and others [2, 3].
The above-mentioned facts highlight the need for broad-spectrum antiviral strategies to design effective universal drugs for easy use in family and clinical practice as a first line of defense for the human population and attending physicians against such highly pathogenic viruses. For example, mortality risks of highly pathogenic influenza viruses of the H5 subtype in humans are estimated at >50% [4, 5], which is similar to the Spanish flu pandemic situation in 1918–1919, with 50–100 million deaths globally [6]. Thus, respiratory viral infections and future pandemics are major global public healthcare problems, and healthcare systems must remain prepared on a global scale for potential viral mutations that can alter viral adaptation and pathogenicity for humans, increase viral transmission patterns from birds and animals to the human population, and initiate the pandemic process.
TYPES OF ANTIVIRAL DRUGS Currently, the arsenal of antiviral agents consists of two major groups:VTA(virus-targetingantivirals)andHTA(host-targeting antivirals). The first group consists of substances that directly target viral proteins or the viral genome, inhibiting viral replication and viral suppressive mechanisms acting on the cellulardefenseresponse.Thesetargetsincludeviralfunctional proteins and RNAs (polymerases, receptor proteins, viral ion channels, viral proteases, viral mRNAs, etc.) and structural viral proteins involved in the morphogenesis and assembly of viral particles. The best-known representatives of this VTA class include rimantadine, baloxavir, oseltamivir, Relenza, favipiravir, ribavirin, molnupiravir, miRNA, recombinant nanobodies, and others used to treat RNA-containing viruses, including influenza and coronavirus infections in humans [7-12]. The VTA class of drugs has two major limitations: (i) a narrow spectrum of specific activity against closely related viruses due to significant virus-specific genomic variations, even among similar viruses, and (ii) the rapid development of viral resistance to such drugs.
This resistance develops due to the high genetic error rate of polymerases of RNA-genomic respiratory viruses, amounting to 10-3–10-4 mutations per round of viral genome replication and producing extremely high amounts of viral quasi-species [13-14]. The second group consists of HTA compounds, which act on cellular targets. This group of drugs is characterized by a wide spectrum of activity against many viruses and a high barrier to resistance due to the inability of viruses to quickly adapt to new host cell metabolism [15-19]. However, this class of compounds acting on the host has an achievable obstacle due to potential cellular toxicity and, consequently, a narrow therapeutic dose window. Nevertheless, these drugs seem to be particularly valuable in the acute phase of respiratory diseases with short treatment courses.
The development of this chemotherapeutic class is realized through several major avenues: (1) inhibitors of cellular receptors used by viruses for penetration into target cells; (2) inhibitors of cellular protein kinases that regulate cellular pathways used by viruses for their replication but do not interfere with defensive cellular processes against viruses; (3) drugs targeting host nucleotide biosynthesis, restricting viral replication and decreasing the emergence of virus drug-resistant mutants; (4) inhibitors of lipid biosynthesis and membrane biogenesis, interfering with viral entry, replication, and viral assembly on lipid membrane rafts; (5) inhibitors of host helicases involved in cellular regulation and IRES-dependent translation of viral mRNA in host cells; and (6) natural and synthetic inhibitors of hostspecific proteases involved in the maturation of viral proteins and activation of viral particle infectivity [11, 20-24].
Currently, this HTA research direction is widely developed and is superior to the traditional “magic bullet” approach discovered by P. Ehrlich at the beginning of the 20th century [25]. BINARY ANTIVIRAL DRUGS AND INHALATION DELIVERY We previously studied the antiviral activity of aprotinin, a lowmolecular-weight polypeptide inhibitor of a broad spectrum of serine proteases [26, 27]. This protease inhibitor was found to demonstrate a marked inhibitory effect (i) on the virus itself, preventing its activation from a non-infectious to an infectious form [20, 28-34] and (ii) on host processes involved in the activation of thrombocyte receptor 1, epithelial Na+ channel (ENaC), kallikrein-activated kinins, and proinflammatory cytokines such as IL-6, TNF-α, thereby reducing clinical thrombosis, coagulation abnormalities, lung edema, and inflammation [35-47].
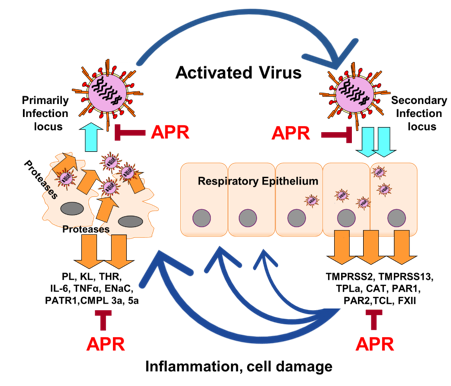
Both inhibitory activities (VTA and HTA) of aprotinin proved to be useful for its therapeutic effects in the body. Aprotinin was proposed as the first binary chemotherapeutic agent possessing a combined VTA-HTA mechanism [20]. The scheme of proteolytic activation of the influenza virus and the binary therapeutic mechanism of aprotinin are illustrated in Fig. 1. Clinical studies conducted in Russia and Spain between 1990 and 2024 demonstrated the antiviral and therapeutic efficacy of aprotinin inhalations in patients suffering from acute respiratory infections caused by influenza viruses, paramyxoviruses, adenoviruses, coronaviruses and others [29, 46, 48-54]. Figure 1. “Vicious cycle” developing influenza pathogenesis and aprotinin targets. Virus stimulates hot proteases, which is one of the necessary factor of virus multicycle replication and influenza pathogenesis.
Up-regulated host activate cellular fusogenic activity and infectivity of synthesized virus through the specific cleavage of the viral receptor protein hemagglutinin HA0 (m.w. 80 kD) into two subunits HA1 (55 kD) and HA2 (25 kD) [20]. Virus-induced cell damage provokes inflammation that induces a leakage of plasmin, kallikrein, thrombin and transcytosis of leucocytes into tissues causing inflammatory processes. Aprotinin suppressing host proteases normalizes proteolytic balance in the infected organism, decreases a spread of virus and development of inflammation to provide multivalent therapeutic action. Designations: KL (kallikrein), PL (plasmin), THR (thrombin), PATR1 (protease-activated thrombocyte receptor 1), ENaC (epithelial Na+ channel), TMPRSS2, TMPRSS13 (transmembrane serine protease 2, and 13), uPA (urokinase plasminogen activator), CMPL 3a, 5a (protease-activated compliment components 3a and 5a), TNF-α (tumor necrosis factor alpha), CAT (cathepsins), TCL (secretory bronchiolar serine protease - Tryptase Clara), PAR1,2 (proteases activating receptors 1 and 2).
There are many ways to further modernize binary drugs through numerous combinations of different agents acting on multiple cellular and viral targets [21, 22, 55, 56]. Such drug combinations will further enhance their synergistic therapeutic efficacy and antiviral spectrum against a wide range of viruses, while reducing therapeutic dosages and side effects. These properties of combined drug formulations will be particularly useful in the fight against new, unknown viral challenges, including avian influenza, highly pathogenic coronaviruses, and novel, still unknown viruses [57-59]. One real threat of this nature currently exists in the form of highly pathogenic variants of the avian influenza virus, predominantly viral hemagglutinin HA antigenic subtypes H5 and H7 containing a highly cleavable multibasic proteolytic site [60-62].
Influenza viruses are maintained in natural avian reservoirs, including aquatic bird species. From this reservoir, the viruses are transmitted to other migratory birds, domestic poultry, swine, cows, and a variety of other mammals. There is a risk that the avian influenza virus will adapt to humans and cause a pandemic with unpredictable consequences [5]. To counter this threat, it is necessary to have highly effective drugs with reasonable and predictable therapeutic and antiviral efficacy in the official arsenal, available in the general healthcare system. One such possibility is demonstrated in Figs. 2 and 3. The figures show an assay of aprotinin, a protease inhibitor, combined with ribavirin, a viral polymerase inhibitor.
Both of these drugs have been approved for clinical use in humans [20, 63, 64]. This drug combination affects multiple targets in viral replication and disease pathogenesis [8, 30, 65-67]. Four daily 7.5-min aerosol inhalations of low dosages of this combination provided achievable therapeutic efficacy in a mouse model of infection caused by the highly pathogenic avian influenza virus subtype H7N2, analogous to the modern avian influenza virus subtype H5N1. Furthermore, this treatment reduced the most serious generalized syndrome of avian influenza-virus dissemination in the infected host and its penetration into the mouse brain. It is important to mention that the inhalation delivery doses used provided high antiviral concentrations in the respiratory epithelial lining fluid, and these doses were more than 100 times lower than toxic concentrations for animals and humans (see the legend to Fig.
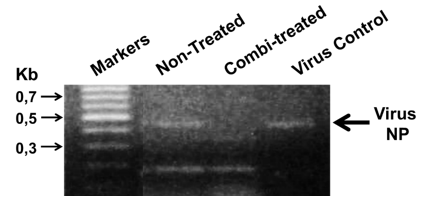
2). Figure 2. Effective inhalation therapy using a mixed aerosol of aprotinin and ribavirin in mice infected with the highly pathogenic avian influenza virus. Mice (25-28 g) infected with the highly pathogenic avian influenza A/chicken/New Jersey/294598/04 (H7N2) virus were given four 8-min inhalations daily of a finely dispersed solution containing a combination of protease inhibitor (aprotinin - 0.3 mg/ml) and ribavirin (8 mg/ml), a combination therapy, or placebo (no drug aerosol treatment), for 4 days. This aerosol inhalation regimen provides 31.5 μg/g/day and 1.5 μg/g/day dosages for ribavirin and aprotinin, respectively. These doses correspond to 2.6 mg/ kg/day and 0.15 mg/kg/day for ribavirin and aprotinin aerosol inhalation dosages in humans, which provides concentration in alveolar lining fluid is 30-60 times the half maximal response (EC50) of about 25 μg/ml (ribavirin) and 70 μg/ml (aprotinin) observed against virus in cultured Caco2 cells test [65; 66].
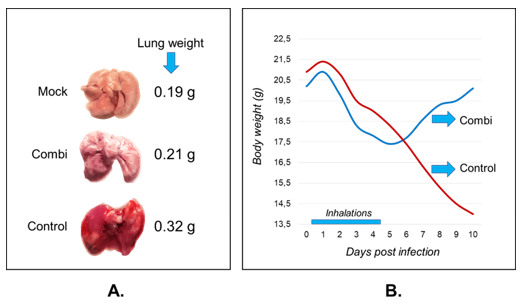
Four days after the start of treatment, the mouse brain was removed, and RNA was isolated from the brain. Viral RNA was determined using a highly sensitive reverse transcriptase reaction (RT- PCR) and PCR with virus-specific primers for the viral NP gene, followed by analysis of the PCR product using agarose gel electrophoresis [68]. The figure shows the presence of the analyzed major viral gene NP (nucleoprotein) product (MW 0.470 kb) in the brain of control mice and its absence in the brain of mice receiving aprotinin-ribavirin combination treatment. Additionally, as shown in Fig. 3, combined aerosol treatment of mice infected with a lethal dose of the mouse-adapted highly pathogenic H7N2 avian influenza virus had a significant positive effect on disease dynamics: it significantly reduced lung inflammation, improved animal weight gain dynamics, and prevented mouse death.
These data propose a prototype for an effective treatment approach against lethal avian influenza, which is known to cause a 60–90% mortality rate in humans [5, 69]. Developed combination therapies with rational multivalent action on a range of viral and cellular targets represent an attractive avenue for creating an effective class of drugs against the highly dangerous threat to humans that could arise should a similar epidemic variant of the avian influenza virus emerge in nature, capable of infecting humans via aerosol transmission. Currently, such variants of the highly pathogenic H5N1 influenza virus have emerged in nature only in certain mammalian species, such as cats, seals, sea lions, foxes, minks, cows, fur animals, etc., and domestic birds.
[4, 5]. There is a real, high risk of such a virus adapting to and spreading among humans. If this scenario occurs, the designed combination therapy could be used as the first line of defense for the urgent protection of humans. Figure 3. Therapeutic efficacy of inhalations with an aerosolized mix of aprotinin and ribavirin in mice infected with the highly pathogenic H7N2 avian influenza virus. Mice (3 mice in each group) infected with highly pathogenic avian influenza virus A/chicken/New Jersey/294598/04 (H7N2) were given combined aprotinin-ribavirin inhalations for 4 days beginning on 12 hrs after infection, as described in the fig.2. On the day 6 after infection, the lungs were removed, weighed, and photographed (left panel A).
The right panel B shows the mouse body weight daily dynamics of treated (Combi) and NoDrug-treated control (Control) mice. FUTURE MODERNIZATION OF BINARY ANTIVIRAL DRUGS Thenextstepinthemodernizationofaprotinin-basedbinarydrugsinvolvedthedevelopmentofapressurizedmanualmetered-dose inhaler (pMDI) containing the ozone-saving fluorocarbon propellant 134A. This propellant has several undesirable technological challenges, including the poor solubility of propellant A134 in aqueous solutions used to prepare the aprotinin polypeptide substance, as well as the possible inactivation of the aprotinin protein structure in the propellant mixture of the designed pressurized inhaler. All these limitations were successfully resolved by a three-component composition comprising propellant, ethanol, and glycerin [70], which was adapted for this aprotinin-containing inhaler. The resulting first compact manual metereddose inhaler, containing polypeptide aprotinin as the active pharmacological substance, passed technical and clinical trials in Russia and was approved under the trademark AERUSR for clinical use in the treatment of acute respiratory viral infections [20].
In the modern era, the concept of novel unknown infectious diseases posing a threat to society, so-called “X” diseases, has emerged [2, 3, 5]. Examples of such pathogens include highly pathogenic avian influenza viruses of the H5 and H7 subtypes, which cause mortality rates of 50–90% in animals and humans, highly lethal coronavirus strains, and the highly pathogenic monkeypox virus. Combating such types of new, unknown viral diseases requires broad-spectrum, multitargeted antiviral drugs as a necessary first line of defense to prevent, or at least reduce, the widespread transmission of these pathogens and high human mortality. In this area, we are developing a binary aerosol drug with two broadspectrum active substances, for example, aprotinin and ribavirin, each of which is approved for clinical use in humans in the US, Canada, and Russia [20, 63, 64].
The initial pilot study conducted on mice infected with the highly pathogenic avian influenza virus supports this approach, demonstrating the high efficacy of this chemotherapeutic combination, as shown above in Figs. 2 and 3. ThesedataallowMDIstobeconsideredforrapidindividualized medication for each patient at the earliest stages of illness and for early prophylactic use in family and hospital practices. MDI devices are currently undergoing development and improvement in several areas. First, new types of propellants are being developed that do not emit CO2 and are completely harmless to the ozone layer, so-called green inhalers [71-75]. The first prototypes of such MDIs have already been approved for clinical trials [76]. Second, the use of nanobiotechnology in aerosol formulations allows for the employment of various types of nanoparticles with absorbed active substances, which stabilize aerosolized mixtures, enable targeted delivery of active substances to specific respiratory sections, including the distal domains of the respiratory tract, and provide prolonged therapeutic effects [77-79].
Third, advances in inhalation devices, including pressurized metered-dose inhalers (pMDIs), dry powder inhalers (DPIs), and different types of nebulizers, have established the pulmonary route for administering biologics, such as biologically active enzymes and peptide molecules, monoclonal antibodies, nanobodies, and their combinations. These devices, delivering inhaled biologics, optimize multivalent therapeutic mechanisms of drugs with their targets and reduce effective dosages and side effects [20, 78-80].
Conclusion
(i) The respiratory infection process caused by viruses, such as influenza viruses, coronaviruses, paramyxoviruses, etc., develops through the mechanism of a “vicious cycle”. The virus activates host proteases, and upregulated proteases activate virus-dependent cell fusion and infectivity of the synthesized virus to promote the spread of infection. On the other hand, cell damage and an overbalance of host proteases, such as plasmin, kallikrein, thrombin, transmembrane serine proteases, PAR1, TMPRSS2, TMPRSS13, uPA, matriptase, tissue plasminogen activator, etc., provoke pathogenic inflammatory processes, lung edema, hyperactive coagulation, thrombosis, and other pathogenic mechanisms. (ii) The exogenous protease inhibitor aprotinin, which suppresses a wide spectrum of proteases, normalizes the host proteolytic balance, decreases the spread of viral infection and the development of inflammation, and provides a marked therapeutic effect.
(iii) A combination of virus-targeted and host-targeted drugs, known as binary drugs, for example, ribavirin, an inhibitor of viral polymerases, and aprotinin, a protease inhibitor, provides protection against highly pathogenic avian influenza virus at low drug dosages and prevents virus dissemination throughout the infected organism. (iv) These binary drug combinations, possessing a wide spectrum of antiviral activity, are proposed for use in handheld metered-dose inhalers (MDIs) as effective drugs for the first line of defense against future new, unknown highly pathogenic viruses, referred to as diseases “X”. (v) The global healthcare system must remain prepared for the high potential risks of natural virus “X” mutations that can dramatically increase viral pathogenicity in humans and viral transmission from birds and animals to the human population, thereby initiating a new pandemic process.
Financial support The author declares the absence of any financial support for this research and publication. Competing interests The author declares no known competing financial interests or personal relationships that could influence the work reported in this article. Acknowledgement The author sincerely thanks Alena Chernyshova for her help with the figure preparation and experimental assistance and prof. A.D.Altstein for his support of my work and valuable discussions. English language editing was kindly provided by English Proofreading Experts (https://english-proofreadingexperts.com).
Figures and Tables
References
- World Health Organization The Top 10 Causes of Death. Aug, 2024. (accessed on 12 September 2024). Available online: https://www.who.int/news-room/fact-sheets/ detail/the-top-10-causes-of-death.
- Simpson S, Kaufmann MC, Glozman V, Chakrabarti A. Disease X: accelerating the development of medical countermeasures for the next pandemic. Lancet Infect Dis. 2020 May;20(5):e108-115. doi: 10.1016/S1473- 3099(20)30123-7. Epub 2020 Mar 17. Erratum in: Lancet Infect Dis. 2020 Dec; 20(12):e298. doi: 10.1016/ S1473-3099(20)30829-X. PMID: 32197097; PMCID: PMC7158580.
- Jiang S, Shi ZL. The First Disease X is Caused by a Highly Transmissible Acute Respiratory Syndrome Coronavirus. Virol Sin. 2020 Jun;35(3):263-265. doi: 10.1007/s12250-020-00206-5 Epub 2020 Feb 14. PMID: 32060789; PMCID: PMC7091198.
- Shi J, Zeng X, Cui P, Yan C, Chen H. Alarming situation of emerging H5 and H7 avian influenza and effective control strategies. Emerg Microbes Infect. 2023 Dec;12(1):2155072. doi: 10.1080/22221751.2022.2155072 PMID: 36458831; PMCID: PMC9754034.
- Zhirnov OP, Lvov DK. Avian flu: «for whom the bell tolls»? Vopr Virusol. 2024May 6;69(2):101-118. doi: 10.36233/10.36233/0507-4088-213 PMID: 38843017.
- Johnson NP, Mueller J. Updating the accounts: global mortality of the 1918-1920 "Spanish" influenza pandemic. Bull Hist Med. 2002 Spring;76(1):105-15. doi: 10.1353/bhm.2002.0022 PMID: 11875246.
- Hayden FG, Shindo N. Influenza virus polymerase inhibitors in clinical development. Curr Opin Infect Dis. 2019 Apr;32(2):176-186. doi: 10.1097/ QCO.0000000000000532. PMID: 30724789; PMCID: PMC6416007.
- Zhirnov O.P., Chernyshova A.I. Favipiravir: the hidden threat of mutagenic action. Journal of microbiology, epidemiology and immunobiology. 2021; 98(2): 213– 220. DOI: https://doi.org/10.36233/0372-9311-114
- Beigel JH, Hayden FG. Influenza Therapeutics in Clinical Practice-Challenges and Recent Advances. Cold Spring Harb Perspect Med. 2021 Apr 1;11(4):a038463. doi: 10.1101/cshperspect.a038463 PMID: 32041763; PMCID: PMC8015700.
- Batool S, Chokkakula S, Song MS. Influenza Treatment: Limitations of Antiviral Therapy and Advantages of Drug Combination Therapy. Microorganisms. 2023 Jan 11;11(1):183. doi: 10.3390/microorganisms11010183 PMID: 36677475; PMCID: PMC9865513.
- Luong QXT, Hoang PT, Ho PT, Ayun RQ, Lee TK, Lee S. PotentialBroad-SpectrumAntiviralAgents:AKeyArsenal Against Newly Emerging and Reemerging Respiratory RNA Viruses. Int J Mol Sci. 2025 Feb 10;26(4):1481. PMC11855616.
- Bayurova E, Kostyushev D, Tikhonov A, Chulanov V, Gordeychuk I. Broad-acting antivirals: the pursuit of pan-viral therapeutics in the era of pandemics. J Virol. 2026 Mar 23:e0007726. doi: 10.1128/jvi.00077-26 Epub ahead of print. PMID: 41870078.
- Sanjuán R, Domingo-Calap P. Mechanisms of viral mutation. Cell Mol Life Sci. 2016 Dec;73(23):4433-4448. 27392606; PMCID: PMC5075021.
- Ison MG, Hayden FG, Hay AJ, Gubareva LV, Govorkova EA, Takashita E, McKimm- Breschkin JL. Influenza polymerase inhibitor resistance: Assessment of the current state of the art - A report of the isirv Antiviral group. Antiviral Res. 2021 Oct;194:105158. doi: 10.1016/j.antiviral.2021.105158 Epub 2021 Aug 4. PMID: 34363859; PMCID: PMC9012257.
- Sepúlveda CS, García CC, Damonte EB. Inhibitors of Nucleotide Biosynthesis as Candidates for a Wide Spectrum of Antiviral Chemotherapy. Microorganisms. 2022 Aug 12;10(8):1631. doi: 10.3390/ microorganisms10081631. PMID: 36014049; PMCID: PMC9413629.
- Roa-Linares VC, Escudero-Flórez M, Vicente- Manzanares M, Gallego-Gómez JC. Host Cell Targets for Unconventional Antivirals against RNA Viruses. Viruses. 2023 Mar 17;15(3):776. doi: 10.3390/v15030776 PMID: 36992484; PMCID: PMC10058429.
- Schreiber A, Ludwig S. Host-targeted antivirals against SARS-CoV-2 in clinical development - Prospect or disappointment? Antiviral Res. 2025 Mar;235:106101. PMID: 39923941.
- Chen Y, Shi Y, Zuo X, Dong X, Xiao X, Chen L, Xiang Z, Ren L, Zhou Z, Wei W, Lei X, Wang J. UNC0638 inhibits SARS- CoV-2 entry by blocking cathepsin L maturation. J Virol. 2025 Jul 22;99(7):e0074125. doi: 10.1128/jvi.00741- 25. Epub 2025 Jun 18. PMID: 40530850; PMCID: PMC12282183.
- Alalem N, Alalem M, Awad A, Elshamy AM, Elalem OR, Tabl AM, Ebaid ME, Khalil H. A novel mechanistic study on inhibiting influenza A virus replication by a newly extracted polypeptide targeting host autophagy. Arch Microbiol. 2025 Sep 18;207(11):267. doi: 10.1007/ s00203-025-04476-z. PMID: 40965660.
- Zhirnov OP, Klenk HD, Wright PF. Aprotinin and similar protease inhibitors as drugs against influenza. Antiviral Res. 2011 Oct;92(1):27-36. doi:10.1016/j antiviral.2011.07.014. Epub 2011 Jul 23. PMID: 21802447. 21. de León P, Cañas-Arranz R, Bustos MJ, Sáiz M, Sobrino F. Inhibition of Human Coronaviruses by Combinations of Host-Targeted and Direct-Acting Antivirals. Antimicrob Agents Chemother. 2023 Apr 18;67(4):e0170322. doi: 10.1128/aac.01703-22 Epub 2023 Mar 28. PMID: 36975844; PMCID: PMC10112268.
- Ludwig S, Pleschka S, Planz O. MEK inhibitors as novel host-targeted antivirals with a dual-benefit mode of action against hyperinflammatory respiratory viral diseases. Curr Opin Virol. 2023 Apr; 59:101304. doi: 10.1016/j.coviro.2023.101304 Epub 2023 Feb
- PMID: 36841033; PMCID: PMC10091867. 23. Beran RK, Vijjapurapu A, Nair V, Du Pont V. Host-targeted antivirals as broad-spectrum inhibitors of respiratory viruses. Curr Opin Virol. 2025 Dec;73:101492. doi: 10.1016/j.coviro.2025.101492 Epub 2025 Oct 1. PMID: 41037996. 24. Wang Y, Wang X, Doğan T, Sam-Agudu NA, Al-Tawfiq JA, Pan Q. Mpox: disease manifestations and therapeutic development. J Virol. 2025 Sep 23;99(9):e0015225. 40787989; PMCID: PMC12459235.
- Schwartz RS. Paul Ehrlich's magic bullets. N Engl J Med. 2004 Mar 11;350(11):1079-80. doi: 10.1056/ NEJMp048021. PMID: 15014180.
- Fritz H, Wunderer G. Biochemistry and applications of aprotinin, the kallikrein inhibitor from bovine organs. Arzneimittelforschung. 1983;33(4):479-94. PMID: 6191764.
- Wegner J. Biochemistry of serine protease inhibitors and their mechanisms of action: a review. J Extra Corpor Technol. 2003 Dec;35(4):326-38. PMID: 14979425.
- Zhirnov OP, Ikizler MR, Wright PF. Cleavage of influenza a virus hemagglutinin in human respiratory epithelium is cell associated and sensitive to exogenous antiproteases. J Virol. 2002 Sep;76(17):8682-9. doi: 10.1128/jvi.76.17.8682-8689.2002 PMID: 12163588; PMCID: PMC136409.
- Zhirnov OP, Matrosovich TY, Matrosovich MN, Klenk HD. Aprotinin, a protease inhibitor, suppresses proteolytic activation of pandemic H1N1v influenza virus. Antivir Chem Chemother. 2011 Mar 7;21(4):169-74. doi: 10.3851/IMP1715
- Böttcher-Friebertshäuser E, Garten W, Matrosovich M, Klenk HD. The hemagglutinin: a determinant of pathogenicity. Curr Top Microbiol Immunol. 2014;385:3- 34. doi: 10.1007/82_2014_384 PMID: 25031010
- Hoffmann M, Kleine-Weber H, Schroeder S. et al. SARS- CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell. 2020 Apr 16;181(2):271-280.e8. doi: 10.1016/j cell.2020.02.052. Epub 2020 Mar 5. PMID: 32142651; PMCID: PMC7102627.
- Bojkova D, Bechtel M, McLaughlin KM, McGreig JE. Et al. Aprotinin Inhibits SARS-CoV-2 Replication. Cells. 2020 Oct 30;9(11):2377. doi: 10.3390/cells9112377 PMID: 33143316; PMCID: PMC7692688.
- Kaur U, Chakrabarti SS, Ojha B, Pathak BK, Singh A, Saso L, Chakrabarti S. Targeting Host Cell Proteases to Prevent SARS-CoV-2 Invasion. Curr Drug Targets. 2021;22(2):192-201. doi: 10.2174/138945012166620092 4113243. PMID: 32972339.
- Presley efficacy against SARS-CoV-2 (JN.1) and influenza A (H1N1) viruses protect mice from influenza A infection. Emerg Microbes Infect. 2026 Dec;15(1):2616944. doi: 10.1080/22221751.2026.2616944 Epub 2026 Jan 30. PMID: 41612887; PMCID: PMC12862872.
- Zhirnov OP. The phenomenon of proteolytic activation of myxoviruses and a new strategy for treating viral diseases. Vopr Virusol. 1983 Jul-Aug;28(4):9-21. Russian. PMID: 6314677.
- Ascenzi P, Bocedi A, Bolognesi M, Spallarossa A, Coletta M, De Cristofaro R,Menegatti E. The bovine basic pancreatic trypsin inhibitor (Kunitz inhibitor): a milestone protein. Curr Protein Pept Sci. 2003 Jun;4(3):231-51. doi:10.2174/1389203033487180 PMID: 12769721.
- Waxler B, Rabito SF. Aprotinin: a serine protease inhibitor with therapeutic actions: its interaction with ACE inhibitors. Curr Pharm Des. 2003;9(9):777-87. doi: 10.2174/1381612033455468 PMID: 12570794.
- Levy JH, Sypniewski E. Aprotinin: a pharmacologic overview. Orthopedics. 2004 Jun;27(6 Suppl):s653-8.
- Moreau ME, Garbacki N, Molinaro G, Brown NJ, Marceau F, Adam A. The kallikrein-kinin system: current and future pharmacological targets. J Pharmacol Sci. 2005 Sep;99(1):6-38. doi: 10.1254/jphs.srj05001x PMID: 16177542.
- Day JR, Landis RC, Taylor KM. Aprotinin and the protease-activated receptor 1 thrombin receptor: antithrombosis, inflammation, and stroke reduction. Semin Cardiothorac Vasc Anesth. 2006 Jun;10(2):132- 42. doi: 10.1177/1089253206288997 PMID: 16959740. (Aprotinin multi: antithrombosis, antiinflammation, antistroke)
- Planès C, Caughey GH. Regulation of the epithelial Na+ channel by peptidases. Curr Top Dev Biol. 2007;78:23- 46. doi: 10.1016/S0070-2153(06)78002-4. PMID: 17338914; PMCID: PMC2276519.
- Landis C. Pharmacologic strategies for combating the inflammatory response. J Extra Corpor Technol. 2007 Dec;39(4):291-5. PMID: 18293823; PMCID: PMC4680701.
- Zhirnov O.P., Poyarkov S., Malyshev N.A. Antiviral and anti-inflammatory targets of aprotinin: Prospects for new uses. Pulmonology. 2009; (3):109-118. https://doi org/10.18093/0869-0189-2009-3-109-118
- Smith M, Kocher HM, Hunt BJ. Aprotinin in severe acute pancreatitis. Int J Clin Pract. 2010 Jan;64(1):84-92. doi: 10.1111/j.1742-1241.2008.01899.x Epub 2009 Jan 28. PMID: 19178597.
- Brown JR, Toler AW, Kramer RS, Landis RC. Antiinflammatory effect of aprotinin: a meta-analysis. J Extra Corpor Technol. 2009 Jun;41(2):79-86. PMID: 19681304; PMCID: PMC4680210.
- Padín JF, Pérez-Ortiz JM, Redondo-Calvo FJ. Aprotinin (I): Understanding the Role of Host Proteases in COVID-19 and the Importance of Pharmacologically Regulating Their Function. Int J Mol Sci. 2024 Jul 10;25(14):7553. PMC11277036.
- Vanglabeke LLW, Rex S, Van den Eynde R. Plateletsparing properties of aprotinin: A scoping review on mechanisms and clinical effects. Eur J Anaesthesiol. 2025 Jan 1;42(1):36-43. doi: 10.1097/EJA.0000000000002081 Epub 2024 Oct 11. PMID: 39628415.
- Zhirnov OP. High protection of animals lethally infected with influenza virus by aprotinin-rimantadine combination. J Med Virol. 1987 Feb;21(2):161-7. doi: 10.1002/jmv.1890210208 PMID: 2434613; PMCID: PMC7166978.
- Ovcharenko AV, Zhirnov OP. Aprotinin aerosol treatment of influenza and paramyxovirus bronchopneumonia of mice. Antiviral Res. 1994 Feb;23(2):107-18. doi: 10.1016/0166-3542(94)90038-8. PMID: 7511880.
- Zhirnov OP, Kirzhner LS, Ovcharenko AV, Malyshev NA. The pathogenetic therapy of acute respiratory diseases by aprotinin inhalations. Ter Arkh. 1995; 67(6):38-42. Russian. PMID: 7545316.
- Zhirnov O.P., Kirzhner L.S., Ovcharenko A.V., Malyshev N.A. Aerosolized aprotinin is an effective drug against viral respiratory illness. Antiinfective Drugs and Chemotherapy. 1996, Vol. 14, No. 3, pages 209-216.
- Zhirnov OP, Bokova NO, Isaeva EI, Vorobieva IV, Malyshev NA. Pathogenetic treatment of influenza patients with aerosolized form of aprotinin, a protease inhibitor. Biopharmaceuticals (Russian) 2015; v.4: 59–64.
- Redondo-Calvo FJ, Padín JF, Muñoz-Rodríguez JR, Serrano-Oviedo L. et al. Aprotinin treatment against SARS-CoV-2: A randomized phase III study to evaluate the safety and efficacy of a pan-protease inhibitor for moderate COVID-19. Eur J Clin Invest. 2022 Jun;52(6):e13776. doi: 10.1111/eci.13776 Epub 2022 Apr 5. PMID: 35342931; PMCID: PMC9111659.
- Redondo-Calvo FJ, Padín JF, Martínez-Alarcón J, et al. Inhaled aprotinin reduces viral load in mild-to-moderate inpatients with SARS-CoV-2 infection. Eur J Clin Invest. 2022;52:e13850. doi: 10.1111/eci.13850
- Wagoner J, Herring S, Hsiang TY, Ianevski A. et al. Combinations of Host- and Virus-Targeting Antiviral Drugs Confer Synergistic Suppression of SARS-CoV-2. Microbiol Spectr. 2022 Oct 26;10(5):e0333122. doi: 10.1128/spectrum.03331-22 Epub 2022 Oct 3. PMID: 36190406; PMCID: PMC9718484.
- Kainov DE, Ravlo E, Ianevski A. Seeking innovative concepts in development of antiviral drug combinations. Antiviral Res. 2025 Feb;234:106079. doi: 10.1016/j antiviral.2025.106079.Epub2025Jan9.PMID:39798882.
- Jiang S, Shi ZL. The First Disease X is Caused by a Highly Transmissible Acute Respiratory Syndrome Coronavirus. Virol Sin. 2020 Jun;35(3):263-265. doi: 10.1007/s12250-020-00206-5 Epub 2020 Feb 14. PMID: 32060789; PMCID: PMC7091198.
- Simpson S, Kaufmann MC, Glozman V, Chakrabarti A. Disease X: accelerating the development of medical countermeasures for the next pandemic. Lancet Infect Dis. 2020 May;20(5):e108-e115. doi: 10.1016/S1473- 3099(20)30123-7. Epub 2020 Mar 17. Erratum in: Lancet Infect Dis. 2020 Dec;20(12):e298. doi: 10.1016/ S1473-3099(20)30829-X. PMID: 32197097; PMCID: PMC7158580.
- Zaman MH, Ali N and Ilyas M. 2024. “Disease X” and prevention policies. Front. Public Health 12:1303584.
- Luczo JM, Spackman E. Molecular Evolution of the H5 and H7 Highly Pathogenic Avian Influenza Virus Haemagglutinin Cleavage Site Motif. Rev Med Virol. 2025 Jan;35(1):e70012. doi: 10.1002/rmv.70012 PMID: 39730318; PMCID: PMC11680514.
- Neumann G, Eisfeld AJ, Kawaoka Y. Viral factors underlying the pandemic potential of influenza viruses. Microbiol Mol Biol Rev. 2025 Jun 25;89(2):e0006624. 40340558; PMCID: PMC12188719.
- Bellido-Martín B, Rijnink WF, Iervolino M, Kuiken T, Richard M, Fouchier RAM. Evolution, spread and impact ofhighlypathogenicH5avianinfluenzaAviruses.NatRev Microbiol. 2026 Jan;24(1):45-60. doi: 10.1038/s41579- 025-01189-4. Epub 2025 May 22. PMID: 40404976.
- Virasole (ribavirin for inhalation solution, USP) prescribibg information (package insert). Bridge-water, NJ: Bauch Health US, LLC; 2019.
- Virasole (ribavirin for inhalation) Solution, USP (product monograph). Leval, Quebec, Canada: Bausch Health Canada Inc; 2020.
- Zhirnov OP. Molecular Targets in the Chemotherapy of Coronavirus Infection. Biochemistry (Mosc). 2020 May;85(5):523-530. doi: 10.1134/S0006297920050016 PMID: 32571182; PMCID: PMC7232917.
- Messina E, Danise A, Ferrari G, Andolina A, Chiurlo M, Razanakolona M, Barakat M, Israel RJ, Castagna A. Ribavirin Aerosol in the Treatment of SARS- CoV-2: A Case Series. Infect Dis Ther. 2021 Dec;10(4):2791-2804. PMID: 34302258; PMCID: PMC8302211.
- Ivashchenko AA, Zagribelnyy BA, Ivanenkov YA, Ivashchenko IA, Karapetian RN, Kravchenko DV, Savchuk NP, Yakubova EV, Ivachtchenko AV. The Efficacy of Aprotinin Combinations with Selected Antiviral Drugs in Mouse Models of Influenza Pneumonia and Coronavirus Infection Caused by SARS-CoV-2. Molecules. 2022 Aug 5;27(15):4975. doi: 10.3390/molecules27154975 PMID: 35956925; PMCID: PMC9370800.
- Zhirnov OP, Chernyshova AI. The uncleaved viral hemagglutinin HA0 increases influenza A virus resistance to thermal pasteurization. Virology. 2025 Mar;604:110389. doi: 10.1016/j.virol.2025.110389 Epub 2025 Jan 3. PMID: 39889479.
- Bartlett ML, Palese P, Davis MF, Vermund SH et al. Enhancing the response to avian influenza in the US and globally. Lancet Reg Health Am. 2025 Apr 28;46:101100. PMCID: PMC12230410.
- Ganderton D, Lewis D, Davies R, Meakin B, Brambilla G, Church T. Modulite: a means of designing the aerosols generated by pressurized metered dose inhalers. Respir Med. 2002 Aug;96 Suppl D:S3-8. doi: 10.1016/s0954- 6111(02)80018-x. PMID: 12201079.
- Salvadori M, Singh D, Mathews K, Girardello L, Cortellini M, Emirova A, Pacchetti I, Foti M, Puviani V, Poli G, Rony F. The low global warming potential propellant HFA- 152a does not induce bronchoconstriction or impair mucociliary clearance. Pulm Pharmacol Ther. 2025 Jun;89:102358. doi: 10.1016/j.pupt.2025.102358 Epub 2025 Apr 5. PMID: 40194694.
- Duke DJ, Rao L, Myatt B, Cocks P, Stein S, Marasini N, Ong HX, Young P. In- vitro Evaluation of Solution Pressurised Metered Dose Inhaler Sprays with Low- GWP Propellants. Pharm Res. 2025 Feb;42(2):385-400. PMID: 39939559; PMCID PMC11880099.
- Wilkinson AJK, Smith LE, Woodcock A. Green inhalers: reducing the carbon footprint of asthma care. Curr Opin Pulm Med. 2026 May 1; 32(3): 239-244. doi: 10.1097/ MCP.0000000000001252. Epub 2026 Feb 11. PMID: 41670025.
- Marasini N, Rao R, Duke D, Myatt B, Cocks P, Stein SW, Traini D, Young P, Ong HX. Development and in vitro evaluation of solution-based pressurized metered- dose inhaler formulations using green propellants. J Pharm Pharmacol. 2026 Feb 6;78(2):rgag005. doi: 10.1093/jpp/ rgag005. PMID: 41697881.
- Singh D, Mancini L, Melis G, Cortellini M, Rostello C, Mathews KS. Safety and tolerability of the low global warming potential propellant HFA-152a in patients with asthma receiving beclometasone dipropionate/ formoterol fumarate/glycopyrronium: The TRECOS study. Respir Med. 2026 May;256:108814. doi: 10.1016/j rmed.2026.108814. Epub 2026 Apr 6. PMID: 41951188.
- “Trixeo Aerosphere” approved in the UK as first inhaled respiratory medicine using next-generation propellant with near-zero global warming potential. Accessed August 18, 2025. https://www.astrazeneca.com/ media-centre/press-releases/2025/trixeo-aerosphereapproved-in-the-uk-as-first-inhaled-respiratorymedicine-using-next-generation-propellant-with-nearzero-global-warming-potential.html
- Barve M. H, Shardul P. K, Munne S. S, Bendale A. R, Naphade V, Pathan V. T, Borse L. B. Metered Dose Inhalers (MDI’S) for High-Performance Pulmonary Drug Delivery in Assistance to Nanotechnology. Biosci Biotech Res Asia 2023;20(2). Available at: https://bit.ly/442AvCT
- Weers JG, Tarara TE, Miller DP. Reimagining Carrier- Based Formulations for Inhalation: Respirable Agglomerates. J Pharm Sci. 2026 Apr 18:104289. doi: 10.1016/j.xphs.2026.104289 PMID: 42009165.
- Mahmoud DE, Hosseini SH, Rathore HA, Alkilany AM, Heise A, Elhissi A. Inhalable Nanotechnology-Based Drug Delivery Systems for the Treatment of Inflammatory Lung Diseases. Pharmaceutics. 2025 Jul 9;17(7):893. doi: 10.3390/pharmaceutics17070893 PMID: 40733101; PMCID: PMC12298333.
- Shaibie NA, Mohammad Faizal NDF, Buang F, Srichana T, Mohd Amin MCI. Inhaled biologics for respiratory diseases: clinical potential and emerging technologies. Drug Deliv Transl Res. 2025 Nov;15(11):4098-4114. Erratum in: Drug Deliv Transl Res. 2026 Jan;16(1):414. PMCID: PMC12508015.
This is a text version generated from the article. For the formatted version of record (with original tables & figures), download the PDF →