Full Text Hide / show
Introduction
AA amyloidosis is a rare disorder, with an incidence of 1 to 2 cases per million people. It arises as a response to chronic inflammation, frequently associated with infections, autoimmune or autoinflammatory diseases; hence, its designation as reactive amyloidosis. It is characterized by an abnormal folding of soluble precursor proteins into a beta-sheet structure, which subsequently deposits in the extracellular space as fibrillar material resistant to proteolytic enzymes. These deposits are derived from serum amyloid A (SAA), an acute-phase reactant produced by hepatocytes under the regulation of proinflammatory cytokines. Persistent overproduction of SAA is essential for the development of AA amyloidosis; however, for reasons not yet fully understood, this phenomenon occurs in a small proportion of patients with chronic inflammatory disorders, of which only 1% correspond to cases associated with tuberculosis in developed countries1 ; although, it may be around 25 to 30% in developing countries2 .
Systemic involvement is common, and can affect the skin, soft tissues, peripheral nervous system, gastrointestinal tract, bloodvessels,andvitalorganssuchasthekidneys,heart,lungs, and liver, leading to alterations in both structure and function. The incidence of AA amyloidosis has decreased, mainly in developed countries, due to improved diagnosis and management of chronic diseases and infections1-5 . A definitive diagnosis is provided by a biopsy of the affected tissue, which must show amyloid deposits with high affinity for Congo red staining, and display characteristic birefringence under polarized light. For the diagnosis of the AA subtype of amyloidosis, it is required immunohistochemical analysis with anti-AA antibodies6 . Treatment should focus on controlling the underlying inflammatory cause5,6 . This case report presents a young man who, despite reactivation of tuberculosis, did not seek medical care for a period of nine months, which led to a grave delay in the diagnosis and treatment after the onset of symptoms.
This resulted in progressive disease, malnutrition, functional decline, pulmonary fibrosis, nephrotic syndrome secondary to AA renal amyloidosis requiring dialysis, and a predisposition to infections. Despite the initiation of anti-tuberculosis therapy and all supportive measures, including comprehensive rehabilitation, the patient developed multi-organ failure due to low physiological reserve and accumulated chronic damage, which finally resulted in his death.
Case Report We report here the case of a 31-year-old male patient, with a history of pulmonary tuberculosis that was treated 13 years prior; as well as psychoactive substances consumption (marijuana and cocaine); without other known comorbidities. He presented with a 9-month clinical picture of asthenia, adynamia, weight loss and respiratory symptoms that included progressive dyspnea, wet cough with purulent sputum, nocturnal diaphoresis. He subsequently developed generalized edema progressing to anasarca, foamy urine, and dyspnea at rest, which finally led him to consult to the emergency room of our hospital. On physical examination, his vital signs revealed a blood pressure of 90/60 mmHg, a heart rate of 90 beats per minute, a respiratory rate of 26 breaths per minute, and an oxygen saturation of 80% on room air.
His body mass index was 18 kg/m2 , and he appeared chronically ill, with marked emaciation, pallor, and facial edema. Cardiac examination revealed rhythmic heart sounds; while respiratory sounds were diminished, particularly over the left lung field, with diffuse crackles in both lung fields. He also exhibited ascites and pitting edema in the lower extremities, above to the thighs, which limited ambulation. Given the clinical suspicion of tuberculosis reactivation, sputum smear microscopy was performed, yielding positive results for acid-fast bacilli (AFB) (++). A CT scan of the chest, neck, and abdomen (Figure 1) revealed bilateral pulmonary infiltrates with a tree-in-bud pattern, left fibrothorax, fibrosing changes in the right upper lobe, mediastinal lymphadenopathy,cardiomegaly,andbilateralnephromegaly.
Antitubercular therapy was initiated, with adjustments for renal function impairment (creatinine 5.23 mg/dL and blood urea nitrogen 66.8 mg/dL). Other laboratory findings included hypoalbuminemia (1.4 g/dL); in addition, urinalysis showed a pH of 6.0, specific gravity of 1.020, proteinuria of 500 mg/dL, and urinary sediment with pyuria, but no casts. PCR for mycobacteria in urine was negative. A complete blood count revealed hemoglobin 8.5 g/dL, leukocytes 8,900/mm³ (neutrophils 7,200/mm³, lymphocytes 1,171/mm³, monocytes 258/mm³, eosinophils 9/mm³), and platelets 215,000/mm³. Proteinuria was quantified at 8 g/24 h, consistent with nephrotic syndrome. Further investigations for secondary causes were performed, including normal liver function tests, and negative viral serologies (HIV, hepatitis B surface antigen, hepatitis C antibodies, and syphilis).
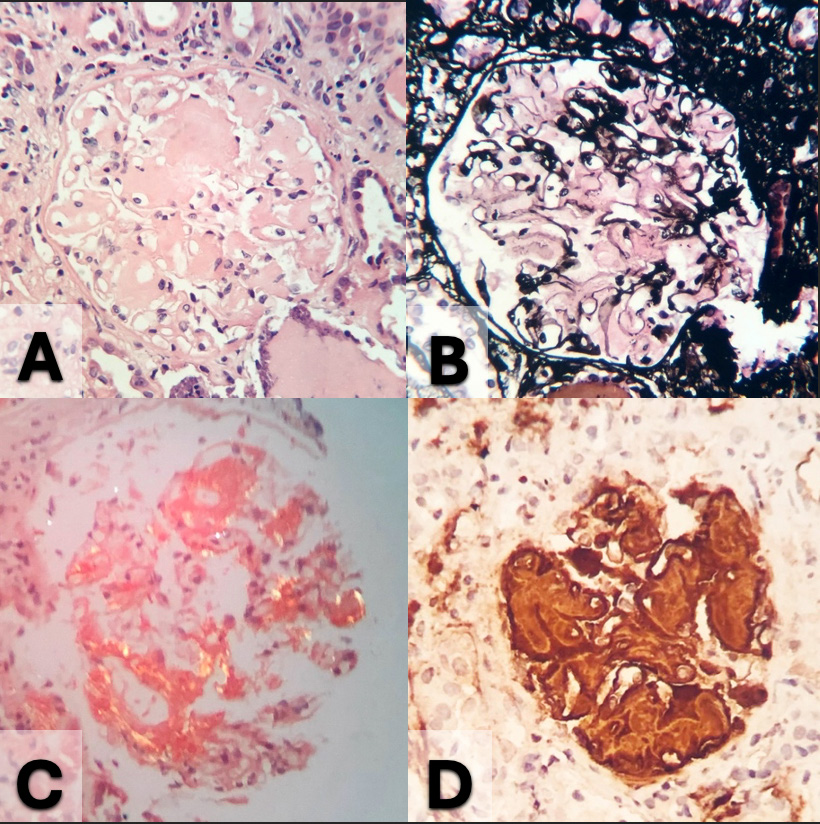
Autoimmune serologies were also negative. Figure 1. Chest X-ray: bilateral pulmonary infiltrates and signs of fibrothorax with predominant left side. Serum protein electrophoresis revealed a faint band in the gamma region. Immunofixation in urine was negative, whereas serum immunofixation showed an IgG Lambda monoclonal component, with a normal kappa/lambda ratio (1.29). However, a bone marrow biopsy was performed without finding paraproteinemia; in addition, it revealed mild normochromic-normocytic anemia, and approximately 4% plasma cells on myelogram, with Congo red staining negative for amyloid. Due to the presence of nephromegaly, the systemic findings, and uncertainty about the chronicity of the renal damage, a renal biopsy was performed (Figure 2). It showed 50% of glomeruli globally sclerosed, with severe mesangial expansion, and capillary wall thickening by acellular, amorphous material, positive for Congo red staining, which indicated amyloidosis.
The interstitium exhibited extensive fibrosis (80%) and tubular atrophy, with amorphous deposits in the vascular walls; it was also positive for Congo red staining. Direct immunofluorescence was negative for IgA, IgG, IgM, C3, C1q, and kappa and lambda light chains. Electron microscopy revealed diffuse podocyte injury with effacement of foot processes and loss of filtration slits. PCR for mycobacteria in renal tissue was negative; mass spectrometry confirmed the diagnosis of renal AA amyloidosis Figure 2. Pathological examination of the kidney. (A) & (B) Glomeruli revealed amorphous deposits in mesangium and capillary walls, viewed H&E 400x (A); and silver stain 400x (B). (C) Congo red stain under polarized light; these deposits show applegreen birefringence 400x.
(D) Diffuse, strong expression of Amyloid AA by immunohistochemistry 400x. In addition, a transthoracic echocardiogram was performed, revealing dilated cardiomyopathy with a left ventricular ejection fraction (LVEF) of 14% and severe eccentric hypertrophy, findings inconsistent with amyloidosis. Cardiac MRI confirmed dilated cardiomyopathy with severe biventricular dysfunction, ruling out infiltrative disease. Chagas disease was also excluded. A diagnosis of cocaine-induced toxic cardiomyopathy was considered. During hospitalization, the patient presented a progressive deterioration of renal function and congestive symptoms, requiring initiation of hemodialysis two weeks after admission. Due to severe heart failure with reduced ejection fraction, and for better hemodynamic tolerance, it was placed a peritoneal dialysis catheter to continue dialysis. Additionally, physical, nutritional, and occupational therapy was started.
Despite these efforts, the patient’s condition continued to decline. He developed complications, including Serratia marcescens peritonitis, bacteremia, pulmonary thromboembolism, and gastrointestinal hemorrhage. Finally, he developed multi-organ failure due to low physiological reserve, accumulated chronic damage and multiple complications, which led to his death.
Discussion
Amyloidosis comprises a group of diseases characterized by abnormal extracellular deposition of insoluble, β-sheet misfolded proteins, known as amyloids. These deposits can disrupt the structure and function of multiple organs and tissues, potentially leading to severe organ failure. Commonly affected organs include the heart, kidneys, liver, spleen, nervous system, and gastrointestinal tract1 . There are more than 30 different types of amyloid proteins that can accumulate in tissues. The most common forms are AL (light-chain) amyloidosis, AA (serum amyloid A) amyloidosis, and ATTR (transthyretin) amyloidosis. Each subtype has a distinct pathogenetic mechanism, and the treatment varies depending on the type of amyloid involved, as well as the extent of organ damage3,7,8 .
Amyloid deposits may affect any organ or system, which results in a wide spectrum of clinical manifestations that are often nonspecific to a type of amyloid, making the diagnosis challenging and frequently delayed. Amyloidosis should be suspected in cases of multiorgan involvement without a clearly defined etiology, which present with symptoms such as unexplained weight loss, exertional dyspnea, peripheral neuropathy, autonomic neuropathy (e.g., postural hypotension, erectile dysfunction, bladder or bowel dysfunction), renal impairment with proteinuria (commonly in the nephrotic range), bilateral carpal tunnel syndrome, hepatomegaly, macroglossia, periorbital purpura, and coagulation abnormalities, among others. It is important to note that cardiac involvement is the main cause of morbidity and mortality, presenting in 50% of cases of AL amyloidosis; and it is a dominant feature in ATTR amyloidosis, although it is infrequent in AA amyloidosis8 , as was the case of our patient where the cardiac involvement was not due to amyloidosis.
The diagnosis of amyloidosis is often made late due to the nonspecific nature of the symptoms, which can vary widely depending on the organs involved. This delay contributes to high mortality, as early diagnosis and treatment are crucial for controlling disease progression5. The diagnosis is based on clinical evidence of organ involvement and histological confirmation of amyloid deposits, typically visualized as amorphous hyaline material under light microscopy, and showing a characteristic green birefringence under polarized light when stained with Congo red 4-6,8 . In the case presented, the diagnosis was late with fatal consequences due to lack of opportunity for medical attention due to social factors. Several cases of AA amyloidosis secondary to pulmonary tuberculosis have been reported in the literature 9-12 .
The present case of AA amyloidosis secondary to disseminated tuberculosis is notable for the prolonged time between symptom onset and diagnosis, as well as delayed treatment initiation, likely due to limited access to medical care. Such delay allowed tuberculosis, in this patient, to follow a natural course; which is a rare event in modern times, given the widespread availability of anti-tuberculosis therapy13 . Although no specific treatment exists for AA amyloidosis, some reports suggest the use of agents such as colchicine, tumor necrosis factor-alpha inhibitors, or eprodisate to reduce inflammation and, consequently, amyloid deposition14-16 . However, the primary therapeutic strategy should focus on addressing the underlying cause of inflammation2,4,6 .
In some cases, regression of amyloid deposits has been observed following the initiation of appropriate antibiotic or antituberculosis therapy17 . Unfortunately, in this patient, the late initiation of treatment, compounded by significant renal involvement (a known marker of poor prognosis 1,18,19,20 ) and complicated by heart failure due to cocaine toxicity, led to a poor outcome. The advanced chronic organ dysfunction, reduced functional reserve, as well as malnutrition, contributed to the patient’s deteriorating condition; which ultimately resulted in a fatal outcome, despite the initiation of anti-tuberculosis therapy and efforts to manage his multiple complications.
Conclusion
AA amyloidosis should be strongly considered in patients with conditions that induce chronic inflammation and exhibit renal involvement of uncertain etiology; particularly, in the presence of nephrotic-range proteinuria. Whenever feasible, histological examination of the affected tissue or organ is crucial, being the kidney the most frequently involved and the most accessible organ for biopsy. The prognosis of AA amyloidosis depends largely on the timeliness of diagnosis and the initiation of treatment, addressing both the amyloid deposition and the underlying chronic inflammatory condition. In certain cases, regression of amyloid deposits has been documented following appropriate therapeutic intervention. In the case here presented, the delay in diagnosis and treatment initiation resulted in multiple complications, that finally culminated with the patient’s death.
Conflicts of Interest
Statement All authors have seen an approved the manuscript. The authors have no conflicts of interest to declare. Acknowledgements: Pablo Tobón Uribe Hospital. Medellín, Colombia; and University of Antioquia. Medellín, Colombia.
Figures and Tables

References
- Lachmann HJ, Goodman HJ, Gilbertson JA, Gallimore JR, Sabin CA, Gillmore JD, Hawkins PN. Natural history and outcome in systemic AA amyloidosis. N Engl J Med 2007, 356(23), 2361–2371. DOI: 10.1056/NEJMoa070265 from NLM.
- Kaaroud H, Harzallah A, Hajji M, Chargui S, Barbouch S, Turki S, Trabelsi R, Goucha R, Ben Moussa F, Ben Maiz H, Ben Hamida F, Abderrahim E. Renal Amyloidosis: Epidemiological, Clinical, and Laboratory Profile in Adults from One Nephrology Center. Int J Nephrol 2022, 2022:8493479. DOI: 10.1155/2022/8493479 from NLM.
- Iadanza MG, Jackson MP, Hewitt EW, Ranson NA, Radford SE. A new era for understanding amyloid structures and disease. Nat Rev Mol Cell Biol 2018, 19(12), 755-773.
- Mirioglu S, Uludag O, Hurdogan O, Kumru G, Berke I, Doumas SA, Frangou E, Gul A. AA Amyloidosis: A Contemporary View. Curr Rheumatol Rep 2024, 26(7), 248-259. DOI: 10.1007/s11926-024-01147-8 from NLM.
- Papa R, Lachmann HJ. Secondary, AA, Amyloidosis. Rheum Dis Clin North Am 2018, ;44(4),585-603. DOI: 10.1016/j.rdc.2018.06.004 from NLM.
- Georgin-Lavialle S, Savey L, Buob D, Bastard JP, Fellahi S, Karras A, Boffa JJ, Grateau G; Collaborators; Audard V, Bridoux F, Damade R, Deshayes S, Giurgea I, Granel B, Hachulla E, Hot A, Jaccard A, Knebelmann B, Marciano S, Pelcot F, Sarrabay G, Boursier G, Sellam J, Terre A, Bourguiba R. French practical guidelines for the diagnosis and management of AA amyloidosis. Rev Med Interne 2023, 44(2), 62-71. DOI: 10.1016/j revmed.2022.12.004 from NLM.
- Gertz MA. Immunoglobulin light chain amyloidosis: 2020 update on diagnosis, prognosis, and treatment. Am J Hematol 2020, 95(7), 848-860. DOI: 10.1002/ajh.25819 from NLM.
- Wechalekar AD, Gillmore JD, Hawkins PN. Systemic amyloidosis. Lancet 2016, 387(10038), 2641-2654. DOI: 10.1016/S0140-6736(15)01274-X from NLM. 9. Öndeş Z, Vayısoğlu Şahin G, Akar H, Aydoğdu Z, Güldaval F. The Diagnosis of Pulmonary Tuberculosis in a Patient with AA Amyloidosis of Unknown Etiology. J Tepecik Educ Res Hosp 2023, 33(2), 273-278. DOI: 10.4274/terh galenos.2022.00378.
- MalikR,PathakN,SharmaS.SecondaryRenalAmyloidosis in Pulmonary Tuberculosis - A Classic Revisited. J Case Rep Stud, 5(4), 404. DOI 10.15744/2348-9820.5.404
- Balwani MR, Kute VB, Shah PR, Wakhare P, Trivedi HL. Secondary renal amyloidosis in a patient of pulmonary tuberculosis and common variable immunodeficiency. J Nephropharmacol 2015, 4(2), 69-71 from NLM.
- El-HennawyAS,GoldsteinM,NicastriA.Renalamyloidosis secondary to tuberculosis of cecum. Nephron 2002, 92(3), 708-710. DOI 10.1159/000064091 from NLM.
- Deshayes S, Aouba A, Grateau G, Georgin-Lavialle S. InfectionsandAAamyloidosis:Anoverview.IntJClinPract 2021, 75(6):e13966. DOI: 10.1111/ijcp.13966 from NLM.
- Escalante A, Ehresmann GR, Quismorio FP Jr. Regression of reactive systemic amyloidosis due to ankylosing spondylitis following the administration of colchicine. Arthritis Rheum 1991, 34(7),920-922. DOI: 10.1002/ art.1780340720 from NLM.
- Gottenberg JE, Merle-Vincent F, Bentaberry F, Allanore Y, Berenbaum F, Fautrel B, Combe B, Durbach A, Sibilia J, Dougados M, Mariette X. Anti-tumor necrosis factor alpha therapy in fifteen patients with AA amyloidosis secondary to inflammatory arthritides: a followup report of tolerability and efficacy. Arthritis Rheum 2003, 48(7), 2019-2024. DOI: 10.1002/art.11163 from NLM.
- Dember LM, Hawkins PN, Hazenberg BP, Gorevic PD, Merlini G, Butrimiene I, Livneh A, Lesnyak O, Puéchal X, Lachmann HJ, Obici L, Balshaw R, Garceau D, Hauck W, Skinner M; Eprodisate for AA Amyloidosis Trial Group. Eprodisate for the treatment of renal disease in AA amyloidosis. N Engl J Med 2007, 356(23), 2349-2360. DOI 10.1056/NEJMoa065644 from NLM.
- Castellano I, Gómez-Martino JR, Hernández MT, Novillo R, Covarsí A. Remission of nephrotic syndrome caused by renal amyloidosis secondary to pulmonary tuberculosis after tuberculostatic treatment. Nefrologia 2001, 21(1), 88-91. PMID: 11344968 from NLM.
- Mohamed N, Nasr SH. Renal Amyloidosis. Surg Pathol Clin 2014, 7(3), 409-425. DOI 10.1016/j.path.2014.04.006 from NLM.
- Gertz MA, Kyle RA. Secondary systemic amyloidosis: responseandsurvivalin64patients.Medicine(Baltimore), 1991, 70(4), 246-256. PMID: 2067409 from NLM.
- Nieto-Ríos JF, Gálvez-Cárdenas KM, García-Prada CA, Aristizabal-Álzate A,Zuluaga-Valencia G, Serna-Higuita LM, et al. Diagnóstico de amiloidosis renal AA mediante espectrometría de masas en un paciente con proceso inflamatorio crónico grave abdominal. Rev. Colomb. Nefrol. 2022; 9(2), e562. https://doi.org/10.22265/ acnef.9.2.562
This is a text version generated from the article. For the formatted version of record (with original tables & figures), download the PDF →