Full Text Hide / show
Introduction
: Nontuberculous Mycobacteria (NTM) constitute a divers distinguished from M. tuberculosis and M. leprae by their inability to cau Although NTM are generally of low pathogenicity, they have the capaci individuals. Clinical case: We present the case of a male native and resident of Alt with Mycobacterium abscessus infection diagnosed by PCR, multi-treate Conclusions: Fistulizing cervical adenitis in an immunocompetent adult raise suspicion of resistant MNT.IL-12 deficiency is an autosomal recessi infections caused by mycobacteria, this mutation was key to the recurren imperative that, in rare and complex cases, we have a multidisciplinary t
Introduction
Nontuberculous Mycobacteria (NTM) constitute a diverse group of bacteria in the genus Mycobacterium. These bacteria are distinguished from M. tuberculosis and M. leprae by their inability to cause tuberculosis or leprosy. These bacteria are ubiquitous in the environment, found mainly in soil and aquatic environments [1,2]. Although NTM are generally of low pathogenicity, they have the capacity to cause opportunistic infections, especially in immunocompromised individuals [1,3]. NTM are classified into two main groups based on their growth speed: Slow-growing and fast-growing. Among slowgrowing species, Mycobacterium Avium complex (MAC) is the most prevalent and is a significant cause of Nontuberculous Mycobacterial Lung Disease (NTM-PD). Conversely, the
nce
N 2831-8129
us Infection In A Patient munodeficiency.
Méndez2, Sandra Kira Niño Oberto2, Nancy Esbeydi a Lizett Zárate Torres4, Jorge Arturo Mayorga Rodríguez n7, Yaxsier de Armas Rodríguez7,8
seases, Mexico. eracruz, Mexico.
. José Barba Rubio” Mexico. n, Mexico. Pathology, University of Guadalajara, Mexico. Havana, Cuba.
se group of bacteria in the genus Mycobacterium. These bacteria are use tuberculosis or leprosy. ity to cause opportunistic infections, especially in immunocompromised
totonga, Veracruz with a primary immunodeficiency in the IL12 receptor ed without a favorable response t that is refractory to antimicrobial and antituberculosis regimens should ive disorder characterized by a predisposition to recurrent and/or severe nt infections, the poor response to treatment, and the fatal outcome. It is team that addresses each area.
Mycobacterium abscessus complex, comprising subspecies such as M. abscessus subsp. abscessus, exemplifies a rapidly expanding NTM and is progressively observed in cystic fibrosis patients. NTM infections can present in diverse forms, ranging from lung disease to disseminated infections, particularly in patients with compromised immune systems [3]. The diagnosis and treatment of NTM infections present significant challenges due to the presence of antibiotic resistance and the absence of a definitive correlation between in vitro susceptibility and clinical outcomes [4,6]. The accurate identification of NTM species is imperative for the effective management of these infections, given the diversity of species and their variability in pathogenicity [7]. These species have been particularly linked to the use of mesotherapy, liposuction, and other cosmetic interventions. Due to their presence in aquatic environments and their
earch unit in Medical Microbiology and Infectious Diseases, Guadalajara, Jalisco,
y-2026 ; Reviewed: 01-June-2026, QC No. AODS - 5778 ;
J. Leonardo Mayorga-Garibaldi
resistance to multiple drugs, these organisms are often difficult to manage, and they have a wide variety of clinical manifestations, including subcutaneous nodules, abscesses, and fistulas. Patients infected with NTM typically present with the following comorbidities: Obesity, gastrointestinal diseases, HIV, Cystic Fibrosis (CF), diabetes mellitus, and asthma, respectively [3,8-10]. The diagnosis of these infections is paramount for determining their prognosis and the appropriate utilization of pharmacology. Consequently, the possession of specific cultures, histopathological studies, and molecular tools that facilitate expeditious identification is of the essence. These tools are instrumental in the rapid assessment of antibiotic resistance profiles, a crucial step in preventing future comorbidities and the onset of psychological and aesthetic sequelae in our patients. Treatment typically necessitates meticulous debridement and the extraction of foreign material. The following drugs are considered to be of use: The following medications are recommended for administration: imipenem (1 g IV every 6 hours), 500 mg of levofloxacin intravenously or orally once daily, 500 mg of clarithromycin orally twice daily, 1 doublestrength tablet of Trimethoprim/Sulfamethoxazole (TMP/ SMX) orally twice daily, 100 to 200 mg of doxycycline orally once daily, 2 g of cefoxitin IV every 6-8 hours, and 10 to 15 mg/kg of amikacin IV once daily It is recommended that combination therapy be administered with at least two drugs that have demonstrated in vitro activity. The duration of therapy is 24 months, with the possibility of an extended period if the infected foreign material persists within the body. Amikacin is typically incorporated into the initial 3 to 6 months of treatment. M. abscessus and M. chelonae are generally resistant to most antibiotics, and they are very difficult or impossible to eradicate. Patients with these infections should be referred to an experienced specialist [11]. Consequently, interdisciplinary efforts among dermatologists, plastic surgeons, and infectious disease specialists are imperative for addressing this issue [12,13].
CLINICAL CASE A 38-year-old man, a bricklayer, residing in Altotonga, Veracruz. His illness began with unintentional weight loss of 5 kilograms over 3 months, diaphoresis, and unquantified fever (predominantly nocturnal), as well as a productive cough in the morning with mucopurulent sputum (small volume, non-foul-smelling). He was evaluated by a private physician, who initiated treatment with unspecified antibiotics, with no clinical improvement. In January 2024, a nodular lesion appeared in the anterior
neck triangle causing dysphagia. (fig 1a, 1b), An ultrasound performed in April 2024 reported cervical lymphadenopathy. A cervical lymph node fine-needle aspiration biopsy was performed on May 25, 2024, with the report noting scant material and keratin. Subsequently, the lesion increased in size, and lesions with the same characteristics appeared on the left side. A biopsy of the skin and soft tissues of the neck was performed (September 6, 2024) due to suspected M. tuberculosis infection, with a report of fistulizing lymphadenitis.
Treatment
with
Dotbal
was
initiated
(September 25, 2024) in the intensive phase, followed by maintenance doses (December 18, 2024), with a partial response. Discharge from the lymph node lesions persisted. He was evaluated at the Infectious Diseases Outpatient Clinic (December 19, 2024), where treatment was initiated with Levofloxacin (750 mg PO every 24 hours) and Linezolid (600 mg PO every 12 hours). He was re-evaluated (January 2025), where it was concluded that there was a “lack of response to treatment” due to the persistence of the described symptoms, the onset of progressive dyspnea (mMrc 2), and increased discharge from the lesions. After 24 hours in the emergency department, he was admitted to the Internal Medicine ward. A treatment regimen was established with amikacin, meropenem, tigecycline, and clarithromycin. At his initial evaluation, he was neurologically intact, with a cylindrical neck, central trachea, visible palpable lymphadenopathy, and fistulas, A purplish nodular lesion measuring approximately 5 cm × 3 cm is observed in the right infraclavicular region; it is tender on palpation, warm, erythematous, soft, not fixed to deeper structures, mobile, and suppurating, with a purulentappearing discharge. Additionally, fistulous lesions are present in cervical regions IV and VI. No relevant laboratory findings were noted upon admission. During the course of the illness, a cervical lymph node biopsy was performed and sent for atypical mycobacterial culture, Zihel-Neelsen stain, (fig 2), and PCR; GenXpert testing of the lymph node reported no TB detected; the patient developed increased oxygen dependency; a chest CT scan was performed, identifying lymph node clusters; a thoracotomy was performed with biopsy sampling, where non-caseating granulomas and acid-fast bacilli were identified. After 15 days of treatment with IV antimicrobials, the fever subsided. The regimen was adjusted by replacing the carbapenem and tetracycline with an oxazolidinone and a fluoroquinolone. However, after 3 days, the patient relapsed with fever and diaphoresis, as well as a tendency toward somnolence, disorientation, and hearing loss. A plain and contrast-enhanced cranial MRI was performed, showing multiple ring-shaped lesions located supra- and infratentorially. No significant findings were noted on targeted questioning. Given the suspicion of primary immunodeficiency, an ELISA test was requested to quantify IL-12 levels, which yielded a value <0.05, well below normal
J. Leonardo Mayorga-Garibaldi
values for this cytokine, confirming the immunodeficiency. A
culture
was
performed
Lowenstein-Jennsen
for
mycobacteria cultured at 35°C, where after 6 days we had the development of a white, cerebriform colony, (fig 3). That we confirmed by the PCR-RFLP technique to be Mycobacterium abscessus as the causative agent. After prolonged treatment with four antibiotic regimens, the patient died.
Conclusions
Fistulizing cervical adenitis in an immunocompetent adult that is refractory to antimicrobial and antituberculosis regimens should raise suspicion of resistant MNT. This case highlights the diagnostic and therapeutic challenges, underscoring the importance of microbiological confirmation and multidisciplinary management to guide targeted therapy. IL-12Rβ1 deficiency is an autosomal recessive disorder
Figure 1a and 1b.- nodular lesions, fistulas at the supra and infrac ⤢ view in PDF
characterized by a predisposition to recurrent and/or severe infections caused by mycobacteria and salmonella, which are otherwise not very pathogenic. IL-12Rβ1 is a receptor chain for both the IL-12 and IL-23 receptors, and its deficiency abolishes signaling from both receptors. This deficiency is due to biallelic mutations in the IL12RB1 gene. [14] In our patient's case, this mutation was key to the recurrent infections, the poor response to treatment, and the fatal outcome. It is imperative that, in rare and complex cases, we have a multidisciplinary team that addresses each area precisely, from the clinical, microbiological, histopathological, and genetic perspectives. We also need coordinated strategies and tools that allow us to increase survival in these types of patients with rare diseases.
clavicular level with drainage of abundant seropurulentmaterial.
J. Leonardo Mayorga-Garibaldi
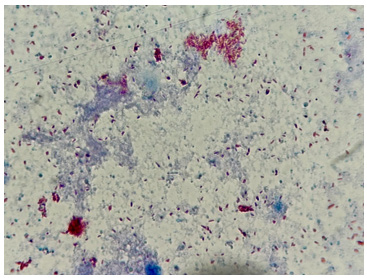
Figure 3.- Lowenstein-jennsen culture with growth of a white, c ⤢ view in PDF
LITERATURE 1.
Claeys TA, Robinson RT. The many lives of nontuberculous mycobacteria. J Bacteriol. 2018; 200: e00739-17.
Tortoli E. Microbiological features and clinical relevance of new species of the genus Mycobacterium. Clin Microbiol Rev. 2014; 27: 727–52.
Jamal F, Hammer MM. Nontuberculous mycobacterial infections. Radiol Clin North Am. 2022; 60: 399–408.
cerebriform colony compatible with Mycobacterium spp.
Yan M, Brode SK, Marras TK. Clinical aspects of lung disease caused by less common slowly growing nontuberculous mycobacteria species. Chest. 2023; 163: 281–291.
Floto RA, Olivier KN, Saiman L, et al. Consensus recommendations for management of non-tuberculous mycobacteria in cystic fibrosis. Thorax. 2016; 71 Suppl 1: i1–22.
Raju RM, Raju SM, Zhao Y, Rubin EJ. Leveraging advances in tuberculosis diagnosis and treatment to address
J. Leonardo Mayorga-Garibaldi
nontuberculous mycobacterial disease. Emerg Infect Dis. 2016; 22: 365–9. 7.
Suresh P, Kumar A, Biswas R, et al. Epidemiology of nontuberculous mycobacterial infection in tuberculosis suspects. Am J Trop Med Hyg. 2021; 105: 1335–1338.
Ma X, Li XY, Liu JW. Demographic and clinical features of nontuberculous mycobacteria infection from cosmetic procedures: a systematic review. Int J Infect Dis. 2024; 149:107259.
Lee MR, Sheng WH, Hung CC, et al. Mycobacterium abscessus complex infections in humans. Emerg Infect Dis. 2015; 21: 1638–46.
10. Leto Barone AA, Grzelak MJ, Frost C, et al. Atypical mycobacterial
infections
after
plastic
surgery
procedures abroad. Ann PlastSurg. 2020; 84: 257–262. 11. Nardell
EA.
tuberculosas.
Infecciones 2022.
por
Available
micobacterias from:
https://
www.msdmanuals.com/es/professional/ enfermedadesinfecciosas/micobacterias/infeccionespor-micobacterias-no-tuberculosas
12. Regnier S, Cambau E, Meningaud JP, et al. Clinical management
rapidly
growing
mycobacterial
cutaneous infections after mesotherapy. Clin Infect Dis. 2009; 49: 1358–64. 13. Gonzalez-Santiago TM, Drage LA. Nontuberculous mycobacteria: skin and soft tissue infections. Dermatol Clin. 2015; 33: 563–77. 14. van de Vosse, E., Haverkamp, M. H., Ramirez-Alejo, N., Martinez-Gallo, M., Blancas-Galicia, L., Metin, A., Garty, B. Z., Sun-Tan, Ç., Broides, A., de Paus, R. A., Keskin, Ö., Çağdaş, D., Tezcan, I., Lopez-Ruzafa, E., Aróstegui, J. I., Levy, J., Espinosa-Rosales, F. J., Sanal, Ö., Santos-Argumedo, L., Casanova, J. L., … Bustamante, J. (2013). IL-12Rβ1 deficiency: mutation update and description of the IL12RB1 variation database. Human mutation, 34(10), 1329–1339. https://doi.org/10.1002/ humu.22380.
Figures and Tables

This is a text version generated from the article. For the formatted version of record (with original tables & figures), download the PDF →