Full Text Hide / show
Introduction
Advance care planning (ACP) is a process that enables individuals to clarify goals and preferences for future medical treatment and care and to discuss them with family members and healthcare providers over time¹. ACP has been associated with improved alignment between patient preferences and end-of-life care and may reduce decisional burden on families². In Japan, national guidelines regarding decision-making in end-of-life care have also emphasized the importance of patient-centered ACP³. Despite its recognized importance, ACP in acute-care settings often remains insufficiently connected to patients’ actual functional conditions and daily-life capabilities. In patients with advanced cancer, changes in physical function, symptom burden, and cognitive status directly influence treatment options, place of care, and end-of-life decisions4.
These observations suggest that ACP should not be regarded as a static, one-time discussion but rather as a dynamic process that evolves alongside the patient’s clinical trajectory. Early integration of palliative care has been shown to improve quality of life and facilitate appropriate decisionmaking in patients with advanced cancer5. Within this context, rehabilitation professionals may play a unique and underrecognized role. Cancer rehabilitation has increasingly been recognized as an essential component of comprehensive oncology and palliative care, particularly for addressing functional impairments throughout the disease trajectory6. By continuously assessing mobility, activity tolerance, and symptom-related limitations, rehabilitation professionals can provide concrete information on the realistic feasibility in daily life7. Such information may help connect patient preferences with practical care decisions.
Our previous systematic–narrative review also suggested that rehabilitation may play an important role in integrating functional assessment and advance care planning within palliative cancer care8. However, clinical evidence describing how rehabilitation professionals contribute to ACP processes in actual patient trajectories remains limited. Nevertheless, the role of rehabilitation in ACP has not been sufficiently explored. Little is known about how rehabilitation involvement interacts with functional trajectories and influences ACP processes in clinical practice. Understanding this relationship may help integrate rehabilitation more effectively into multidisciplinary ACP frameworks. Therefore, this study aimed to explore how rehabilitation professionals contribute to ACP among palliative cancer patients by focusing on functional trajectories and their influence on decision-making processes.
Methods
Study design and setting This study was a retrospective case series conducted at a single acute-care hospital in Japan. The study period covered three consecutive years (2023–2025). Participants We included palliative cancer patients who met the following criteria: (1) received rehabilitation interventions during hospitalization, and (2) had documented advance care planning (ACP)-related decision-making processes in the medical records. Eight patients were identified and included in the analysis (bone metastasis: n = 3; brain metastasis: n = 2; lung cancer: n = 3). Data collection Clinical data were extracted from electronic medical records, including: •Demographic characteristics (age, sex, primary diagnosis) •Functional status (mobility, activities of daily living [ADL], activity tolerance) •Symptom burden (e.g., pain, dyspnea, cognitive changes) •Details of rehabilitation interventions •ACP-related information (treatment preferences, place of care, do-not-attempt-resuscitation [DNAR] decisions, and family involvement) Functional and clinical assessment Functional status was assessed descriptively based on ADL performance, mobility level, and activity tolerance.
Symptom progression was evaluated using routine clinical documentation, with a focus on major symptoms that affect decision-making, such as pain and dyspnea. ACP processes were evaluated by reviewing documented discussions and decisions regarding treatment goals, care settings, and endof-life preferences. Analytical framework Cases were analyzed descriptively and categorized according to functional and clinical trajectories. Four trajectory patterns were identified: 1.Functional decline trajectory 2.Recovery/stabilization trajectory 3.Symptom-driven trajectory 4.Psychological trajectory in the terminal phase Representative cases were selected for each trajectory to illustrate the relationship between rehabilitation involvement and ACP processes. Ethical considerations This study was conducted in accordance with the Declaration of Helsinki and the ethical guidelines for medical and health research involving human subjects in Japan.
As a retrospective study using anonymized clinical data, no additional interventions were performed. Informed consent was waived, and an opt-out approach was used. Information about the study was disclosed through institutional notice and on the website, allowing patients or their proxies to decline to participate. The institutional review board at our hospital approved the study protocol (Approval No. 2026-09).
Results
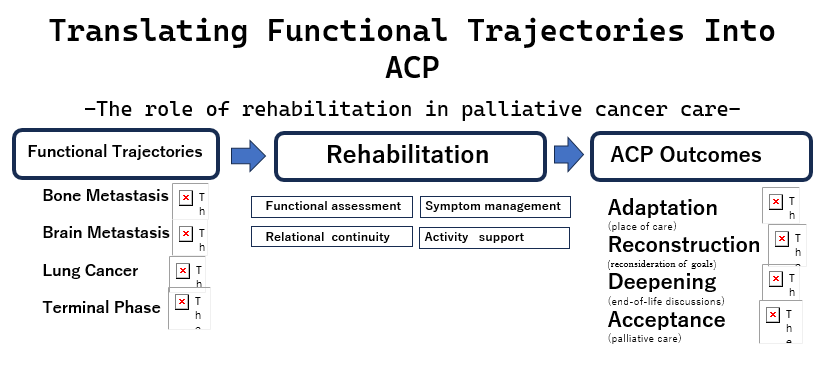
A total of eight patients were included in this study. Based on functional and clinical trajectories, the cases were categorized into four distinct patterns: functional decline, recovery/ stabilization, symptom-driven, and psychological trajectories in the terminal phase (Table 1). These patterns aligned with the conceptual model presented in Figure 1. In all cases, rehabilitation professionals were involved continuously throughout the clinical course, rather than providing episodic interventions. Their longitudinal engagement enabled close monitoring of functional changes, symptom progression, and patient responses, thereby dynamically contributing to ACP processes. Integration with Table 1 and Figure 1 The findings across all cases are summarized in Table 1, which provides an overview of functional trajectories, rehabilitation contributions, and ACP outcomes.
These empirical observations align with the conceptual framework illustrated in Figure 1, demonstrating how different trajectories lead to distinct ACP processes, including adaptation, reconstruction, stabilization, deepening, convergence, concretization, and acceptance. Table 1. Functional trajectories, rehabilitation involvement, and ACP outcomes in palliative cancer patients. 1 Functional Decline Progressive mobility loss due to bone metastasis and severe pain Continuous reassessment of mobility, pain-oriented positioning, transfer support, and communication of realistic home-care limitations Adaptation to hospital-based end-of-life care 2 Functional Decline Pain-driven deterioration caused by spinal metastasis Activity modulation, pain-adapted mobilization, and repeated functional reassessment were shared with the multidisciplinary team Transition to best supportive care 3 Psychological Severe functional decline with existential withdrawal in the terminal phase Relationship-centered bedside involvement focused on emotional stabilization and relational continuity.
Gradual acceptance of palliative care 4 Recovery / Stabilization Functional recovery after treatment for brain metastasis Mobility restoration, activity tolerance support, and facilitation of futureoriented discussions Reconstruction of ACP and reconsideration of treatment goals 5 Recovery / Stabilization Gradual decline after brain metastasis Environmental adjustment and maintenance-oriented support promoting shared understanding with the family Stabilization of ACP 6 Symptom-Driven Progressive dyspnea and anxiety in advanced lung cancer Breathing training, pacing strategies, symptom-oriented rehabilitation, and emotional reassurance Deepening of ACP, including discussions regarding sedation 7 Symptom-Driven Rapid functional deterioration in advanced lung cancer Continuous monitoring of activity tolerance and communication of prognostic changes Rapid convergence of care decisions 8 Symptom-Driven Symptom relief enabling meaningful activities in advanced lung cancer Activity support, mobilization, and facilitation of value-based interactions with family Concretization of patient values into care decisions Figure 1.
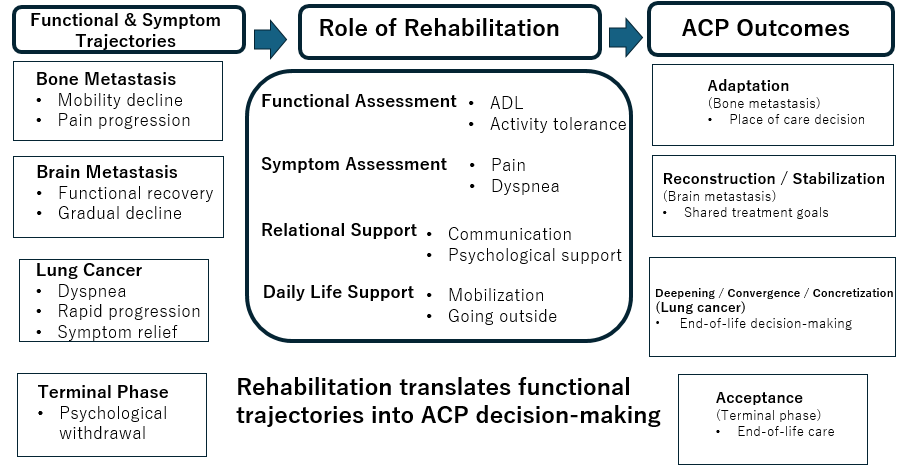
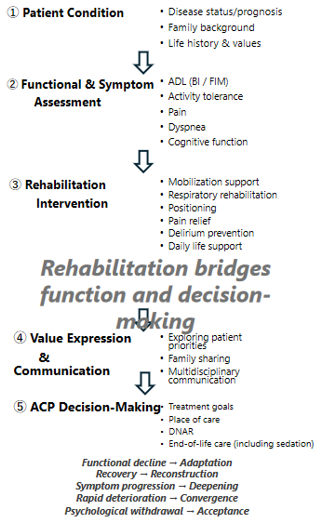
Trajectory-Driven Model of Advance Care Planning Through Rehabilitation in Palliative Cancer Care. This figure illustrates a trajectory-driven model of advance care planning (ACP) in palliative care for cancer. Rehabilitation professionals continuously assess functional status, symptom burden, and psychosocial factors throughout the disease course, translating functional trajectories into meaningful ACP decision-making. Figure 2. Role of Rehabilitation Professionals in ACP Implementation. This figure summarizes the role of rehabilitation professionals in ACP implementation. Through continuous assessment, symptomoriented interventions, and ongoing communication with patients and families, rehabilitation supports the expression of values and patient-centered decision-making. Functional decline trajectory (bone metastasis) Patients with bone metastasis showed progressive mobility decline and increasing pain, which strongly influenced ACP regarding place of care and treatment goals.
Rehabilitation professionals continuously assessed functional deterioration and supported adaptation to realistic care options. REPRESENTATIVE CASE 1 Functional decline trajectory in bone metastasis A woman with advanced uterine cancer and multiple bone metastases was referred to the palliative care team because of progressive pain and functional decline. At the time of rehabilitation initiation, the patient was still able to transfer with assistance and expressed a strong desire to maintain independence in daily activities. Rehabilitation interventions initially focused on maintaining mobility, sitting tolerance, and safe transfer ability. However, progressive spine and pelvic pain gradually limited activity. Rehabilitation professionals continuously adjust interventions in response to symptom fluctuations, including pain-relieving positioning, assisted mobilization, and environmental modifications to reduce physical burden.
During daily rehabilitation sessions, the patients increasingly expressed concerns regarding loss of independence. Statements such as “I can no longer move the way I used to” and “I may not be able to go home” emerged gradually. These expressions were not elicited during formal ACP discussions but rather arose naturally during rehabilitation encounters involving attempts at movement and activity. Rehabilitation staff carefully observed that even brief sitting caused severe pain and fatigue, and that transfer assistance became progressively difficult for family members. These functional observations were repeatedly shared during multidisciplinary conferences, allowing the healthcare team and family to understand the practical implications of disease progression. Importantly, rehabilitation professionals translated abstract functional decline into concrete life-related information.
Rather than simply reporting decreased ADL performance, they explained how deterioration affected realistic daily activities, including toileting, sitting tolerance, and the feasibility of home-based care. This perspective helped bridge the gap between medical prognosis and everyday life expectations. As the disease progressed, the patient’s priorities gradually shifted from maintaining independence to prioritizing comfort and minimizing suffering. Family members also began to recognize the growing physical burden of home care. Through repeated discussions supported by rehabilitation-based functional assessments, the patient and family ultimately chose hospital-based end-of-life care. Although functional recovery was no longer achievable, rehabilitation continued to play an important supportive role until the terminal phase. Interventions focused on comfortoriented positioning, pain reduction during movement, and dignity preservation in daily care.
The patient remained engaged with rehabilitation staff until late in the clinical course, suggesting that rehabilitation contributed not only to physical support but also to maintaining relational continuity during ACP. This case illustrates how progressive functional decline can dynamically reshape ACP. It demonstrates that rehabilitation professionals can facilitate realistic decision-making by continuously translating functional deterioration into meaningful information for patients and families. Recovery/stabilization trajectory (brain metastasis) Patients with brain metastasis demonstrated either functional recovery or gradual decline after treatment. Rehabilitation professionals supported mobility, activity tolerance, and communicationregardingchangingpatientgoals,contributing to the reconstruction or stabilization of the ACP. REPRESENTATIVE CASE 2 Recovery/stabilization trajectory in brain metastasis A woman in her late sixties with advanced breast cancer and brain metastases was admitted with severe functional decline.
At the time of admission, she was almost completely bedridden and required extensive assistance for all activities of daily living. She also exhibited decreased motivation and limited participation in communication regarding future care. Whole-brain radiation therapy was initiated, and rehabilitation interventions began concurrently. Initially, rehabilitation goals were modest and focused primarily on preventing disuse syndrome, ensuring safe positioning, and maintaining sitting tolerance. However, during the early rehabilitation phase, subtle functional improvements became apparent. The patient gradually regained trunk control, maintained sitting posture for longer periods, and eventually achieved assisted standing. Rehabilitation professionals closely monitored these changes and adjusted the intensity of interventions in response to daily fluctuations in fatigue, neurological symptoms, and activity tolerance.
Importantly, rehabilitation sessions became opportunities for the patient to express thoughts and preferences that had not emerged during formal medical discussions. As mobility improved, the patient increasingly verbalized future-oriented wishes, including statements such as “I want to go home once again” and “I would like to spend more time with my family.” These expressions represented a marked shift from the earlier stage characterized by passivity and resignation. Rehabilitation staff recognized that functional recovery was influencing not only physical abilities but also psychological outlook and decision-making capacity. These observations were repeatedly shared during multidisciplinary conferences involving physicians, nurses, medical social workers, and family members. Through this process, previously established assumptions regarding exclusively comfort-focused care began to change.
Thepatientandfamilyreconsideredavailabletreatmentoptions, balancing symptom burden with the possibility of maintaining meaningful daily activities. ACP discussions, therefore, evolved dynamically in response to functional improvements. In addition to physical rehabilitation, therapists supported meaningful activities that reflected the patient’s values and identity. Interventions included encouraging grooming activities, supporting short-distance ambulation within the ward, and facilitating family interaction during rehabilitation sessions. These activities appeared to reinforce the patient’s sense of autonomy and dignity. Although the disease eventually progressed, the patient and family achieved a shared understanding of future care preferences. ACP became more stable and concrete because decisions were grounded in lived experiences of recovery and participationratherthanabstractprognosticdiscussionsalone. This case demonstrates that rehabilitation can influence ACP not only through management of decline but also by creating opportunities for recovery, hope, and re-evaluation of future goals.
Functional improvement may therefore serve as a trigger for ACP reconstruction, highlighting the importance of repeated reassessment throughout the disease trajectory. Symptom-driven trajectory (lung cancer) In patients with lung cancer, dyspnea and symptom burden strongly influence ACP processes. Symptom-oriented rehabilitation supported communication regarding patient values and facilitated trajectory-based decision-making. REPRESENTATIVE CASE 3 Symptom-driven trajectory in advanced lung cancer A patient with advanced lung cancer was referred for rehabilitation because of progressive dyspnea, severe fatigue, and declining activity tolerance. At the time of referral, the patient experienced marked breathlessness even with minimal exertion and spent most of the day in bed. Initially, rehabilitation interventions focused on symptomoriented approaches rather than functional recovery.
Rehabilitation professionals introduced breathing techniques, pacing strategies, positioning adjustments, and low-intensity mobilization to reduce dyspnea-related distress. Interventions were carefully individualized according to daily symptom fluctuations and oxygen demand. During early rehabilitation sessions, the patient repeatedly expressed fear regarding worsening breathlessness and uncertainty about the future. Statements such as “I am afraid I will suffocate” and “I do not know how much longer I can tolerate this” reflected not only physical suffering but also profound psychological and existential distress. Rehabilitation staff maintained close communication during interventions, often pausing sessions to prioritize emotional reassurance and symptom stabilization. Over time, the patient gradually developed trust in the rehabilitation team and became more willing to discuss personal concerns and future wishes during therapy sessions.
As symptom management improved, the patient regained limited but meaningful activity tolerance. Rehabilitation professionals supported short-distance ambulation, sitting activities, and opportunities for interaction with family members outside the patient room. Although these activities were physically modest, they had a significant emotional impact. Notably, rehabilitation sessions became moments when the patient could articulate personal values more concretely. The patient expressed a strong desire to spend meaningful time with family and stated, “I want to remain myself for as long as possible.” These expressions emerged naturally during activity-based interactions rather than during formal ACP meetings. The rehabilitation team shared these observations during multidisciplinary conferences, contributing to deeper ACP discussions among physicians, nurses, family members, and the patient.
As the disease progressed further, dyspnea became increasingly refractory despite pharmacological management. The patient eventually expressed a preference for prioritizing comfort over life-prolonging interventions. Subsequently, discussions regarding palliative sedation were initiated. Importantly, these decisions were not made abruptly at the terminal stage but evolved gradually through repeated rehabilitation encounters, during which symptom burden, activity limitations, and personal values were continuously explored. Even during the late terminal phase, rehabilitation interventions continued in a modified form, focusing on comfort-oriented positioning, breathing support, and maintaining opportunities for communication with family. Rehabilitation professionals remained involved until shortly before death, providing continuity of care and emotional support. This case illustrates that rehabilitation in palliative care extends beyond physical training and may serve as a platform for expressing values and concretizing ACP.
Symptomoriented rehabilitation enabled the patient to reconnect functional experiences with personal meaning, thereby facilitating trajectory-driven decision-making. Psychological trajectory in the terminal phase In terminal-phase patients with psychological withdrawal, rehabilitation professionals focused on relational continuity and emotional stabilization, contributing to acceptanceoriented ACP. REPRESENTATIVE CASE 4 Psychological trajectory in the terminal phase A patient with terminal-stage cancer and extensive metastatic disease was referred for rehabilitation because of severe physical decline, generalized weakness, and psychological withdrawal. At the time of referral, the patient spent most of the day in bed, demonstrated minimal spontaneous activity, and frequently expressed hopelessness regarding both treatment and daily life. Unlike other trajectories in which rehabilitation goals focused on mobility or symptom management, the primary challenge in this case was profound existential and psychological distress.
During early encounters, the patient often responded with short answers and occasionally stated, “Nothing matters anymore” or “There is no point in trying.” Recognizing that direct encouragement toward activity might increase distress, rehabilitation professionals intentionally shifted the focus of intervention from functional improvement to relational continuity. Initial sessions emphasized presence rather than performance. Therapists remained at the bedside, engaged in casual conversation, and explored topics related to the patient’s previous lifestyle, family relationships, and meaningful life experiences. Over time, these repeated interactions gradually reduced emotional tension. Although measurable physical improvement was limited, the patient became increasingly willing to engage in conversation during rehabilitation sessions. Importantly, communication regarding fears, preferences, and concerns emerged naturally within the therapeutic relationship rather than during formal ACP interviews.
The rehabilitation team also paid close attention to subtle behavioral changes, including willingness to sit briefly outside the bed, increased eye contact with family members, and occasional participation in shared activities. These seemingly small changes were interpreted as signs of psychological stabilization and were shared during multidisciplinary conferences. Family members initially struggled to understand the patient’s emotional withdrawal and often interpreted inactivity as “giving up.” Rehabilitation professionals helped family members recognize that maintaining presence, comfort, and emotional connection could itself represent meaningful goals in the terminal phase. This reframing reduced family anxiety and facilitated more supportive communication. As the patient’s condition deteriorated further, rehabilitation interventions became increasingly comfort-oriented. Sessions focused on positioning, minimizing movementrelated distress, and preserving opportunities for interaction with family.
Although the patient rarely initiated explicit discussions about future care, gradual acceptance of the proposed palliative approach was evident in nonverbal responses and decreased resistance to supportive care. Ultimately, the patient accepted transfer to a palliative care unit, where end-of-life care was continued with family support. Rehabilitation professionals remained involved throughout the transition, contributing to continuity and emotional stability. This case highlights that rehabilitation in the terminal phase may function less as a means of restoring function and more as a relational and existential support process. In such situations, rehabilitation professionals may help create the psychological conditions necessary for acceptance-oriented ACP, even when direct decision-making conversations are limited.
Discussion
The present study demonstrated that advance care planning (ACP) in palliative cancer care is not a static, one-time process but rather a dynamic process shaped by functional and clinical trajectories. By analyzing eight cases across four trajectory patterns—functional decline, recovery/stabilization, symptom-driven progression, and psychological changes in the terminal phase, we identified how ongoing rehabilitation involvement influenced ACP processes and outcomes. A key finding of this study is that rehabilitation professionals contributed not only through physical interventions but also through continuous translation of functional changes into meaningful information for decision-making. Because rehabilitation professionals maintain close and repeated contact with patients throughout the course, they are uniquely positioned to observe how mobility, activity tolerance, symptom burden, and psychosocial conditions affect the realistic feasibility of daily life.
This longitudinal involvement enabled rehabilitation to function as a practical bridge between abstract patient preferences and concrete care decisions. In the functional decline trajectory, commonly observed in patients with bone metastasis, progressive mobility loss and increasing pain strongly influenced decisions regarding place of care and treatment goals. Previous studies have demonstrated that functional decline is closely associated with end-of-life transitions and care needs4. In our cases, rehabilitation professionals repeatedly assessed mobility limitations and pain-related restrictions and communicated these findings in terms of practical daily-life implications. This process helped patients and families recognize the feasibility and burden of home-based care, thereby facilitating adaptation-oriented ACP. In contrast, the recovery/stabilization trajectory demonstrated that functional improvement may reshape patient expectations and reconstruct ACP.
ACP has increasingly been conceptualized as an iterative process that should be revisited as clinical conditions change9. In our brain metastasis cases, even modest recovery in mobility and activity tolerance influencedpsychologicaloutlookandfuture-orientedthinking. Rehabilitation sessions became opportunities for patients to express wishes regarding family interaction, home discharge, and meaningful daily activities. These findings suggest that ACP should not be limited to discussions surrounding deterioration alone; recovery experiences may also influence values, goals, and decision-making. The symptom-driven trajectory, particularly in advanced lung cancer, highlighted the importance of symptom-oriented rehabilitation. Dyspnea is known to involve psychological and existential dimensions in addition to physical distress10. In our cases, worsening breathlessness intensified prognostic awareness and prompted discussions regarding comfortfocused care.
Rehabilitation professionals contributed by providing breathing support, pacing strategies, and activity modulation while maintaining close communication with patients and families. These repeated interactions facilitated the expression of value and deepened ACP discussions. Rehabilitation-based goal setting may help patients reconnect meaningful activities with personal values during serious illness 11. The psychological trajectory in the terminal phase illustrated another important dimension of rehabilitation involvement. In patients with profound psychological withdrawal or existential distress, direct participation in ACP discussions was often limited. Previous studies on dignity-conserving care have emphasized the importance of relational continuity and emotional support in end-of-life care12. In our cases, rehabilitation professionals intentionally shifted their focus from functional recovery to supportive presence and emotional stabilization.
Through repeated bedside interactions, they helped foster the gradual acceptance of supportive care and facilitated communication between patients and their family members. These findings suggest that rehabilitation may support ACP even when explicit decision-making conversations are difficult. Taken together, our findings support the concept of ACP as a trajectory-sensitive process influenced by functional status, symptom burden, and psychosocial conditions. While ACP is often discussed primarily as a communication process, effective serious-illness communication remains essential for patient-centered decision-making13. Our findings further suggest that integrating functional assessment into these discussions may improve the practicality and relevance of ACP. Rehabilitation professionals uniquely bridge the gap between abstract preferences and real-life decision-making through continuous functional assessment and patientcentered support.
Our previous review highlighted the conceptual importance of integrating rehabilitation into palliative care and ACP frameworks8. The present case series extends those theoretical perspectives by demonstrating how rehabilitation contributes to ACP processes in actual clinical trajectories. The role of rehabilitation in ACP has received relatively limited attention compared with that of physicians and nurses. However, previous studies have emphasized the importance of multidisciplinary palliative care throughout the cancer trajectory14, as well as the growing role of rehabilitation in advanced cancer care5,6,7,15. Our study further extends these perspectives by demonstrating that rehabilitation contributes not only to symptom management and quality of life but also directly to ACP implementation. From a clinical perspective, incorporating rehabilitation into ACP discussions may help patients and families better understand the practical implications of disease progression and treatment choices.
Continuous rehabilitation involvement may also facilitate timely reassessment of ACP as patient conditions evolve. This study has several limitations. First, it was a retrospective case series conducted at a single institution with a small sample size, limiting generalizability. Second, the analysis was descriptive and did not include a quantitative evaluation of functional outcomes or ACP-related measures. Third, ACP processes were assessed using medical records, which may not fully capture the nuances of patient-family communication and emotional experiences. Despite these limitations, this study provides a clinically relevant framework for understanding how rehabilitation involvement interacts with ACP in palliative cancer care. By focusing on functional trajectories, we demonstrated that rehabilitation can meaningfully contribute to decision-making across different stages of illness.
Future multicenter studies with larger sample sizes are needed to validate these findings and explore quantitative relationships between functional trajectories and ACP outcomes. Development of structured educational programs and multidisciplinary frameworks supporting rehabilitation involvement in ACP may further improve patient-centered palliative care.
Conclusion
ACP in palliative cancer care is a dynamic process shaped by functional trajectories. Rehabilitation professionals contribute uniquely to this process by integrating functional assessment, symptom support, and patient-centered decision-making.
Figures and Tables
| 1 | Functional Decline | Progressive mobility loss due to bone metastasis and severe pain | Continuous reassessment of mobility, pain-oriented positioning, transfer support, and communication of realistic home-care limitations | Adaptation to hospital-based end-of-life care |
|---|---|---|---|---|
| 2 | Functional Decline | Pain-driven deterioration caused by spinal metastasis | Activity modulation, pain-adapted mobilization, and repeated functional reassessment were shared with the multidisciplinary team | Transition to best supportive care |
| 3 | Psychological | Severe functional decline with existential withdrawal in the terminal phase | Relationship-centered bedside involvement focused on emotional stabilization and relational continuity. | Gradual acceptance of palliative care |
| 4 | Recovery / Stabilization | Functional recovery after treatment for brain metastasis | Mobility restoration, activity tolerance support, and facilitation of future- oriented discussions | Reconstruction of ACP and reconsideration of treatment goals |
| 5 | Recovery / Stabilization | Gradual decline after brain metastasis | Environmental adjustment and maintenance-oriented support promoting shared understanding with the family | Stabilization of ACP |
| 6 | Symptom-Driven | Progressive dyspnea and anxiety in advanced lung cancer | Breathing training, pacing strategies, symptom-oriented rehabilitation, and emotional reassurance | Deepening of ACP, including discussions regarding sedation |
| 7 | Symptom-Driven | Rapid functional deterioration in advanced lung cancer | Continuous monitoring of activity tolerance and communication of prognostic changes | Rapid convergence of care decisions |
| 8 | Symptom-Driven | Symptom relief enabling meaningful activities in advanced lung cancer | Activity support, mobilization, and facilitation of value-based interactions with family | Concretization of patient values into care decisions |
References
- Rietjens JAC, Sudore RL, Connolly M, van Delden JJ, Drickamer MA, Droger M, et al. Definition and recommendations for advance care planning: an international consensus. Lancet Oncol. 2017;18:e543– 51. doi: 10.1016/S1470-2045(17)30582-X.
- Brinkman-Stoppelenburg A, Rietjens JA, van der Heide A. The effects of advance care planning on end-of-life care: a systematic review. Palliat Med. 2014;28:1000–25.
- Ministry of Health, Labour and Welfare of Japan. Guidelines for the Decision-Making Process in End-of- Life Care. Tokyo: Ministry of Health, Labour and Welfare; 2018. (in Japanese)
- Gill TM, Gahbauer EA, Han L, Allore HG. Trajectories of disability in the last year of life. N Engl J Med. 2010;362:1173–80. doi: 10.1056/NEJMoa0909087
- Temel JS, Greer JA, Muzikansky A, Gallagher ER, Admane S, Jackson VA, et al. Early palliative care for patients with metastatic non–small-cell lung cancer. N Engl J Med. 2010;363:733–42. doi: 10.1056/NEJMoa1000678
- Silver JK, Baima J, Mayer RS. Impairment-driven cancer rehabilitation: an essential component of quality care and survivorship. CA Cancer J Clin. 2013;63:295–317.
- Cheville AL, Troxel AB, Basford JR, Kornblith AB. Prevalence and treatment patterns of physical impairments in patients with metastatic breast cancer. J Clin Oncol. 2008;26:2621–9. doi: 10.1200/ JCO.2007.12.3075.
- Ohkura S, Sagae S, Someki N, Tanimoto A, Konishi A, Iizuka A et al. Current status and future perspectives of cancer rehabilitation in palliative care: a systematic– narrative hybrid review. Ann Phys Med Rehabil. 2025;14. doi:10.52338/apmr.2025.5180
- Sudore RL, Lum HD, You JJ, Hanson LC, Meier DE, Pantilat SZ, et al. Defining advance care planning for adults: a consensus definition from a multidisciplinary Delphi panel. JAMA Intern Med. 2017;177:1043–49. doi. org/10.1016/j-jpainsymman.2016.12.331
- Ekström MP, Bajwah S, Bland JM, Currow DC, Hussain J, Johnson MJ. One evidence base; three stories: do opioids relieve chronic breathlessness? Thorax. 2018;73:88–90. doi.org/10.1136/thoraxxjnl-2016-209868
- Levack WMM, Weatherall M, Hay-Smith EJC, Dean SG, McPherson K, Siegert RJ. Goal setting and strategies to enhance goal pursuit in adult rehabilitation: summary of a Cochrane systematic review and meta-analysis. Eur J Phys Rehabil Med. 2016;52:400–16. Epub 2016 Jan 15.
- Chochinov HM, McClement S, Hack T, Thompson G, Dufault B, Harlos M. Dignity-conserving care—a new model for palliative care. JAMA. 2002;287:2253–60. doi. org/10.1016/j.jpainsymman.2014.11.291
- Bernacki RE, Block SD; American College of Physicians High Value Care Task Force.Communication about serious illness care goals: a review and synthesis of best practices.JAMA Intern Med. 2014;174:1994–2003. doi: 10.1001/jamainternmed.2014.5271
- Hui D, Bruera E. Integrating palliative care into the trajectory of cancer care.Nat Rev Clin Oncol. 2016;13:159–71. doi:10.1038/nrclinonc.2015.201
- Morishita S, Hamaue Y, Fukushima T, Tanaka T, Fu JB, Nakano J. Effect of Exercise on Mortality and Recurrence in Patients With Cancer: A Systematic Review and Meta-Analysis. Integr Cancer Ther. 2020 Jan-Dec:19:1534735420917462. doi: 10.1177/1534735420917462
This is a text version generated from the article. For the formatted version of record (with original tables & figures), download the PDF →