Full Text Hide / show
Introduction
Facial fat tissue is not a simple “inert filler”; histologically, it is a metabolically active and regionally specialized organ, with direct implications for aging and rejuvenation therapies (1,2). Facial fat is predominantly subcutaneous white adipose tissue organized into lobules of unilocular adipocytes, separated by fibrous septa containing vessels, nerves, and mesenchymal stem cells (3). Only about one‑third of its volume corresponds to mature adipocytes; the remaining two‑thirds is stromal vascular fraction (SVF), composed of preadipocytes, stem cells, fibroblasts, immune cells, and a microvascular network, which confers considerable regenerative and immunomodulatory potential (1). Facial adipocytes show reduced lipolytic responsiveness to β‑adrenergic agonists and a distinct β2/β3 receptor profile, suggesting a more conservative fatty‑acid metabolism with a tendency to preserve volume under basal conditions; these features, together with differences in HOX gene expression, support the concept that facial fat is a functional subtype distinct from other subcutaneous depots (4,5).
Dermal white adipose tissue (dWAT) is an adipose compartment within the deep dermis, whose adipocytes interact intensively with fibroblasts,skinappendages,andthelocalimmunesystem(6). In photoaged skin, a reduction of dWAT and its replacement by fibrosis is observed, associated with adipocyte‑to‑myofibroblast transition (AMT), contributing to stiffness, thinning, and wrinkling. These observations have led to the proposal of dermal adipocytes as therapeutic targets for anti‑aging interventions (bio‑stimulation, energy‑based devices, targeted drugs) (7). As with all adipose tissue, facial fat secretes adipokines and cytokines (leptin, adiponectin, resistin, pro‑inflammatory factors) that act in an autocrine, paracrine, and systemic manner (8). Adipocytes and SVF cells regulate triglyceride storage and release, and respond to insulin, sex hormones, catecholamines, and vitamin D, integrating systemic metabolic signals with local responses in the face (9).
Current evidence indicates that adipose tissue—particularly the superficial panniculus system and, specifically, dermal white adipose tissue—undergoes significant structural changes in its shape and volumetric distribution as the aging process begins (10). In this context, the facial adipoestructuration (FA) technique emerges which, unlike other procedures, aims to reposition tissues in their original anatomical location and algorithmically redistribute structural weight without resection of fat tissue, promoting neocollagenesis and elastogenesis and thereby improving dermal texture, quality, and the paracrine and endocrine response of fat tissue (11). To objectively validate these changes, high‑frequency ultrasound is presented as a fundamental, non‑invasive diagnostic tool that enables in vivo assessment of the pathophysiological aspects of the integumentary system, overcoming the limitations of conventional biopsy and allowing comparison with healthy metabolic profiles.
Operating at frequencies above 10 MHz, this technology provides the resolution needed to identify microstructures and accurately differentiate the epidermal, dermal, and subcutaneous layers (12). This, in turn, makes it possible to monitor the progression of senescence and treatment response by identifying variations in dermal thickness and echogenicity, which directly reflect changes in extracellular matrix density. On this basis, the present study aims to use high‑frequency ultrasonography to evaluate structural changes in the dermoepidermal and hypodermal planes of the malar adipose compartment after application of the facial adipoestructuration (FA) technique, comparing them with ultrasound profiles from different age ranges that characterize metabolic health. Ultrasound can serve as a morpho‑mechanical proxy for the functional state of fat, enabling the assessment of the endocrine behavior of adipose tissue.
Fat tissue, particularly dermal and subdermal white adipose tissue, exerts a metabolic influence on the dermis through a close adipocyte–fibroblast–immune system crosstalk. This layer not only contains skin appendages and deep mechanoreceptors, such as Pacinian and Ruffini corpuscles, but also shares a tight cellular relationship with superficial adipose tissue, since adipocytes and fibroblasts derive from common precursors. This proximity suggests that dermal white adipose tissue (dWAT) plays a crucial role as a cellular reservoir in tissue regeneration and has recently been recognized as an important organ for both metabolic and non‑metabolic health (14). For this reason, it is essential to understand part of the aging process, as scientific evidence indicates that collagen synthesized by fibroblasts does not necessarily decrease due to reduced synthetic activity, but is also affected by collagen catabolism (15).
This prevents its physiological degradation and replacement and instead leads to architectural changes in these fibers. In other words, collagen undergoes a glycation process, defined as the spontaneous reaction of blood glucose with proteins in this case, collagen and elastin fibers which accumulate large amounts of AGEs, the end products of advanced glycation, directly associated with oxidative stress. These AGEs deposit both inside and outside cells, binding to plasma‑membrane proteins, circulating proteins and structural proteins, disrupting the scaffold they form and thereby increasing tissue fragility (16) However, this entire aging process radically alters this architecture. At the molecular level, cellular senescence manifests as an arrest of post‑mitotic proliferation, in which cells begin to secrete the Senescence‑Associated Secretory Phenotype (SASP).
In other words, the cell loses its proliferative capacity but remains metabolically active. This excessive accumulation of senescent cells creates a favorable pro‑inflammatory state known as “inflammaging” (17). These cells are characterized by the complex production and secretion of cytokines, chemokines and matrix metalloproteinases, which establish a pro‑inflammatory microenvironment that degrades the extracellular matrix (18) resulting in dermal atrophy characterized by disorganization of type I, III and IV collagen, degeneration of elastic fibers, and a critical reduction in glycosaminoglycans; factors that clinically manifest as rhytidosis, dehydration and an abnormal redistribution of adipose tissue (10, 19) In this distribution, atrophy becomes evident in the temporal, supraparotid, malar, gonial (or posterior mandibular) and frontal fat pads, whereas the nasolabial and anterior mandibular (submental) fat pads exhibit marked hypertrophy, thereby compromising the balance of facial structure (11).
Regarding these considerations, particular attention is drawn to the superficial adipose compartment of the malar region, which is located along the lateral surface of the zygoma and extends anteriorly toward the paranasal region. It consists of a combination of fibroligamentous adipose tissue and numerous vascular structures that can hinder precise identification of the adjacent subcutaneous plane, and it is characterized by being structurally unstable and atrophic (20). Therefore, it is imperative to validate all structures and their pathophysiological changes through in vivo monitoring, which has advanced thanks to high-resolution ultrasound, as it enables precise identification of the tegumentary layers when frequencies above 10 MHz are used (21). This, in turn, allows qualitative and quantitative visualization through the acquisition of images characterized by their different echogenicities (22).
This makes in-depth evaluation crucial in aging cases, as it allows interpretation of variations in dermal thickness and their associated changes. One of the most notable diagnostic findings is the appearance of the “subepidermal low-echogenic band” (SLEB), which serves as an ultrasonographic biomarker of photoaging and elastosis (23). Ultimately, ultrasonography not only allows characterization of the aging pattern but also becomes the standard tool for quantifying the response to anti-aging treatments (24), in addition to characterizing skin properties across different age ranges (25). Within this framework, intelligent rejuvenation represents the cornerstone of facial adipoestructuring as a regenerative technique designed to restore the original anatomical position of tissues through cannular stimulation and the application of senotherapeutic active principles.
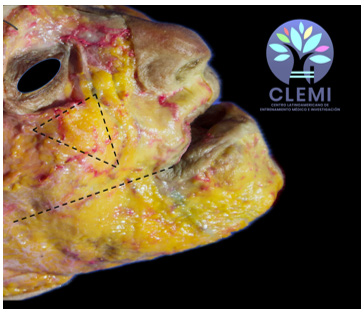
It not only seeks to reverse the state of cellular senescence in terms of its biochemistry and mechanics, but also translates its outcomes into quantitative data to reveal specific parameters at the eco-structural level (11, 25). CLINICAL CASE PRESENTATION A 42-year-old female patient from Valencia, Carabobo State, Venezuela, presented with the chief complaint of aesthetic dissatisfaction due to visible signs of facial aging. During the clinical interview, the facial adipostructuring (FA) protocol, its potential benefits, and post-procedural care were explained in detail. The patient provided authorization by signing an informed consent form, confirming full understanding of the procedure, as well as the associated risks and expected outcomes. Prior to the intervention, a comprehensive facial analysis was performed, including assessment of her facial anatomy (Figure 1), determination of the degree of aging, evaluation of skin quality, and clarification of her expectations as a patient.
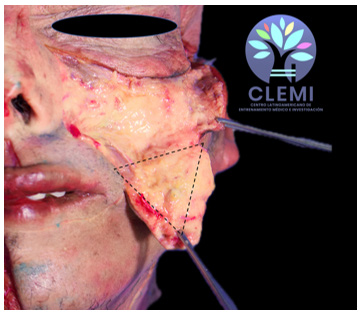
In the malar compartment, the dWAT, through the activity of adipocytes, is capable of releasing fatty acids and adipokines that modify the metabolism of neighboring fibroblasts via their close relationship with adjacent structures (Figure 2). This becomes clinically evident in patients with volumetric deficiency and loss of projection, where clinical findings allow correlation with the histology of the component under evaluation, given the collapse of the compartment and the release of senescenceassociated products. Figure 1. Superficial facial dissection illustrating the position of the malar fat panniculus located below the orbit in the shape of an inverted triangle, delimited by Camper’s plane. Latin American Center for Medical Training and Research (CLEMI), Bogotá, Colombia.
Figure 2. Superficial dissection of the malar fat pad with extension to the mandible and over the Camper plane to observe its structure and length. Latin American Center for Medical Training and Research (CLEMI), Bogotá, Colombia. As part of the documentation protocol, standardized photographic and ultrasonographic images were obtained using a high-resolution, multifrequency ultrasound scanner operating between 16 and 20 MHz (Clarius L20). Although several facial points were analyzed, the study focused specifically on the superficial adipose compartment of the malar region. The facial adipostructuring protocol consisted of three scheduled treatment sessions. At the end of the treatment, a follow-up ultrasonographic assessment was performed in the same anatomical region to evaluate changes in the echogenicity pattern and tissue organization.
MATERIALS AND TECHNIQUE The protocol comprised three sessions at 15-day intervals. The technique was performed using 22G and 25G × 50 mm cannulas to approach the superficial adipose panniculi, and 27G × 50 mm cannulas for ligaments and interseptal spaces. interseptal spaces, using 1 mL syringes loaded with senotherapeutic agents from the FACESTRUCTURE Kit, Mioface Harmony. The systematic procedure included: Antisepsis of the area with 70% alcohol. Cutaneous marking (Face Paint) of the treatment zones. Creation of the entry point with a guiding needle according to the cannula gauge (22G or 25G); mechanical stimulation of the superficial adipose compartments was then performed through three manual stages (3 to 5 movements per vector), followed by deposition of the senotherapeutic agents using a retroinjection technique.
Approach to the interseptal spaces by opening with a 27G needle and insertion of the corresponding cannula, with retroinjection of the senotherapeutic agent without displacement maneuvers. Provision of postoperative instructions to the patient.
Results
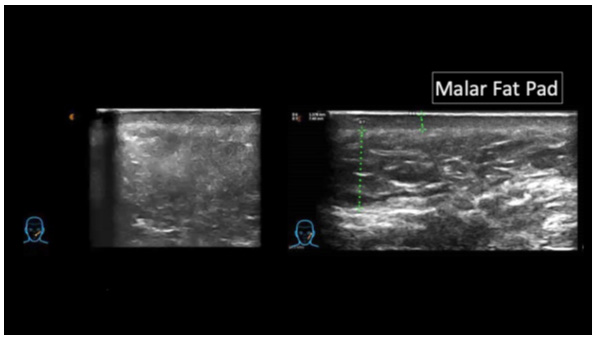
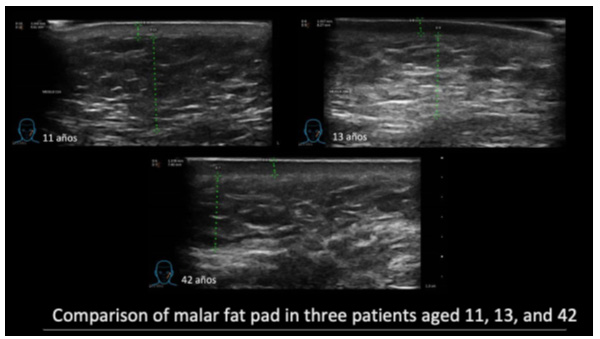
Following completion of the three-session facial adipostructuring (FA) protocol with the FaceStructure kit, highresolution ultrasonographic evaluation revealed significant structural changes in all superficial adipose compartments. Focusing specifically on the malar region compartment, the most relevant finding was a modification in the arrangement pattern of the connective tissue fibers supporting the adipocytes, with evidence of tissue reorganization and a slight increase in echogenicity and eco-structural definition in the treated area (Figure 3). In quantitative terms, Figure 4 shows that, at the dermoepidermal plane in this 42-year-old patient, a posttreatment thickness of 1.378 mm was achieved. When these data were compared with reference profiles, a marked similarity was observed with the thickness values of younger subjects, which measured 1.342 mm (11 years) and 1.557 mm (13 years), respectively.
At the hypodermal plane (Figure 4), the patient exhibited a post-treatment thickness of 7.40 mm. under FA, showing a tendency to approximate the profile of younger subjects (11 years: 9.81 mm; 13 years: 8.27 mm). Likewise, the comparative analysis of the malar panniculus revealed a thickening of the connective tissue fibers, a phenomenon associated with the anatomical repositioning of the tissues (Figure 4). This confirms that the dermal pattern in the treated patient acquired morphological characteristics similar to those observed in the younger age intervals. Figure 3. Ultrasonographic evaluation of the malar panniculus in a 42-year-old female patient, in comparison with the anatomical component of the treated area. Figure 4.
Comparative ultrasound evaluation of the untreated malar panniculus in 11- and 13-year-old patients, compared with the treated area in a 42-year-old patient following facial Adipostructuring.
Discussion
The findings of this study reinforce the role of highfrequency ultrasonography (16–20 MHz) as an objective, non-invasive diagnostic tool for the evaluation of facial regenerative therapies. In line with the literature, while epidermal thickness remains relatively constant (0.15–0.17 mm), the dermis undergoes critical variations; an increase in thickness is described up to the age of 40 years, followed by degenerative processes of the extracellular matrix (26). In this context, the 42-year-old patient initially presented dermal disorganization consistent with this transition toward senescence, in which volume loss and hypocellularity are key histological determinants (25). In contrast to the natural tendency toward thinning and loss of echogenicity after the fourth decade of life, the results obtained following facial adipostructuring (FA) demonstrated a reversal of these parameters.
The patient reached a dermoepidermal thickness of 1.378 mm, a value remarkably close to the profiles of 11-year-old (1.342 mm) and 13-yearold (1.557 mm) subjects. This phenomenon suggests that the FA technique not only mechanically repositions tissues, but also induces a reorganization of collagen and elastin fibers, increasing extracellular matrix density and, consequently, its echogenicity, indicating that histological changes precede visible clinical improvement. Taken together, peridermal fat acts as a metabolic organ that regulatesthedermis:thechangesinducedbyadipostructuring translate into controlled secretion of adipokines or conversion to myofibroblasts that participate in matrix remodeling, elasticity, and a reduction in the rate of cutaneous aging (22). Ultrasound does not directly measure hormone secretion; however, it delineates a “healthier” fat phenotype (improved structure and stiffness) that correlates with a more favorable endocrine profile (12, 22).
In this case, the ability of the Clarius L20 system to detect thickening of connective tissue fibers and modification of ecostructural patterns supports the efficacy of FA before tissue remodeling processes are fully completed. It is noteworthy that the convergence toward thickness values observed in younger age ranges (11–13 years) at both dermoepidermal and hypodermal planes positions FA as an intervention capable of restoring the architecture of dermal white adipose tissue (dWAT), mitigating the disorganization induced by intrinsic and extrinsic factors.
Conclusion
Facial aging is a complex process that transcends the cutaneous surface and originates from a cascade of molecular events, including advanced glycation, oxidative stress, and the establishment of the “inflammaging” phenotype. The transition of dermal cells toward a state of senescence (SASP) not only disorganizes the extracellular matrix, but also alters the dynamics of fat compartments, leading to pathological volumetric redistribution characterized by atrophy of structural panniculi (such as the malar fat pad) and hypertrophy of dependent deposits (such as the nasolabial fat pad). The present investigation demonstrates that facial adipostructuring (FA) represents a paradigm shift in facial rejuvenation. Unlike other techniques, it acts on the cellular microenvironment to reverse senescence, restore the lipolytic–lipogenic balance, and drive tissue reorganization that promotes neocollagenesis and elastogenesis while maintaining the metabolic equilibrium of facial adipose tissue.
Finally, high-frequency ultrasonography is reaffirmed as the gold standard tool for facial harmonization. Its ability to identify biomarkers and monitor in vivo changes by providing images comparable to histology consolidates an evidencebased scientific approach, enabling precise quantification of tissue regeneration. DISCLOSURES Human subjects: Informed consent was obtained from all participants in this study for treatment and open-access publication, or such consent was waived as appropriate. Conflicts of interest: All authors declare the following. Payment/services information: All authors have stated that they received no financial support from any organization for the work submitted. Financial relationships: All authors have declared that they have no financial relationships, either currently or within the past three years, with any organizations that might have an interest in the work submitted.
Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the work presented.
Figures and Tables
References
- Sbarbati A, Accorsi D, Benati D, Marchetti L, Orsini G, Rigotti G, Panettiere P. (2010).Subcutaneous adipose tissue classification. Eur J Histochem. 25;54(4):e48. PMC3167328.
- Hinte LC, Ghosh A, Castellano-Castillo D, Wolfrum C, von Meyenn F. (2010) An epigenome atlas of mouse adipocytes. Mol Metab.99:102197. doi: 10.1016/j molmet.2025.102197. Epub 2025 Jun 27. PMID: 40582590; PMCID: PMC12274702.
- Constantin G, Marconi S, Rossi B, Angiari S, Calderan L, Anghileri E, et al.(2009) Adipose-derived mesenchymal stemcellsamelioratechronicexperimentalautoimmune encephalomyelitis. Stem Cells. 27:2624–35. doi: 10.1002/ stem.194.
- Wollina U, Wetzker R, Abdel-Naser MB, Kruglikov IL. (2017). Role of adipose tissue in facial aging. Clin Interv Aging. 6;12:2069-2076. doi: 10.2147/CIA.S151599 PMID: 29255352; PMCID: PMC5723114.
- Chon SH, Pappas A. (2014). Differentiation and characterization of human facial subcutaneous adipocytes. Adipocyte. 14;4(1):13-21. doi: 10.4161/21623945.2014.955402 eCollection 2015 Jan- Mar.
- Skin aging: Are adipocytes the next target? Ilja L. Kruglikov, Philipp E. Scherer Cell BiologyInternal MedicineInt Med - Touchstone Diab Ctr
- Kruglikov IL, Scherer PE. (2016) Skin aging: are adipocytes the next target? Aging (Albany NY). 8(7):1457-69. doi: 10.18632/aging.100999 PMID: 27434510; PMCID: PMC4993342.
- Stella X. Chen, Ling-Juan Zhang, Richard L. Gallo, (2019). Dermal White Adipose Tissue: A Newly Recognized Layer of Skin Innate Defense, Journal of Investigative Dermatology, Volume 139, Issue 5, 1002-1009, ISSN 0022-202X,
- K.-J. Chung, M. Nati, T. Chavakis, A. (2018). ChatzigeorgiouInnate immune cells in the adipose tissue,Rev Endocr Metab Disord, 19 pp. 283-292
- Uitto, J. (2008). El papel de la elastina y el colágeno en el envejecimiento cutáneo: envejecimiento intrínseco versus fotoexposición. J Drugs Dermatol;7:s12-6.
- Velazco, GJ; Suárez-Vega, DV; Solórzano, EA; Mercado, V; Amin, M. (2025). Análisis estructural del tejido sometido a la técnica de adipoestructuración facial: Un estudio histológico. J Cutan Aesthet Surg. doi: 10.25259/ JCAS_201_2025
- Crisan, D., Lupsor, M., Boca, A., Crisan, M., & Badea, R. (2012). Ultrasonographic assessment of skin structure according to age. Indian journal of dermatology, venereology and leprology, 78, 519.
- Arda, O., Göksügür, N., & Tüzün, Y. (2014). Estructura histológica básica y funciones de la piel facial. Clinics in dermatology , 32 (1), 3-13.
- Liu M , Lu F , Feng J. Envejecimiento y homeostasis de la hipodermis en el deterioro de la función cutánea relacionado con laedad. Cell Death Dis . 2024; 15 : 443 .
- Elizabeth, S. P., Alejandro, S. A., & Pedro, D. R. (2018). Caracterización histológica y morfométrica de la piel facial en personas mayores de 40 años de la provincia Holguín. In morfovirtual2018.
- Ibarra, L., & Camacho, R. (2023). Adipoestructuración facial: una nueva herramienta para la armonización orofacial. Secuencia de casos. Acta Bioclinica, 13(26), 95-115.
- Alcalá-Pérez, D., Cobos-Lladó, D. E., & Santa-Cruz, F. J. (2019). «Inflammaging»: envejecimiento inflamatorio. Revista del Centro Dermatológico Pascua, 27(3), 87-91.
- Maciel-Barón, L. Á., Pérez, V. I., Torres, C., González- Puertos,V.Y.,Konigsberg,M.,&López-Diazguerrero,N.E. (2017).Lasenescenciacelularcomodenominadorcomún de enfermedades asociadas a la edad. Revista Médica del Instituto Mexicano del Seguro Social, 55(4), 490-497.
- Pineda,Z.M.R.,Rivera,I.,Ollarves,V.,Lugo,D.A.,&Hagel, I. (2021). Aspectos moleculares del envejecimiento cutáneo. Dermatología Venezolana, 59(2).
- Schenck TL, Koban KC, Schlattau A. et al. (2018). Updated anatomy of the buccal space and its implications for plastic, reconstructive and aesthetic procedures. J Plast Reconstr Aesthetic Surg; 71(2): 162–70.
- Cammarota, T., Pinto, F., Magliaro, A., & Sarno, A. (1998). Usos actuales de la ecografía diagnóstica de alta frecuencia en dermatología. Revista europea de radiología , 27 , S215-S223.
- Velazco, G; Herrera, A; Gutiérrez, JH, (2026). High- Resolution Ultrasound-Guided Facial Adipose Tissue Restructuring: A Precise Approach to Rejuvenation in a Clinical Case. Cureus. 8;18(3). doi: 10.7759/ cureus.104848. PMID: 41952928; PMCID: PMC13055567.
- Pastor, M (2014).Ecografía en el paciente cosmético, Cutaneous sonography of cosmetic patient. Servicio de Dermatología Hospital Arnau de Vilanova. Valencia Actual. Med; 99: (793). Supl. 60-68.
- Gniadecka M. (2001). Efectos del envejecimiento en la ecogenicidad dérmica. Skin Res Technol;7:204-7.
- Gniadecka, M & Jemec, G. (1998). Evaluación cuantitativa del envejecimiento cronológico y el fotoenvejecimiento in vivo : Estudios sobre la ecogenicidad y el grosor de la piel. Br J Dermatol;139:815-21.
- Pineda,Z.M.R.,Rivera,I.,Ollarves,V.,Lugo,D.A.,&Hagel, I. (2021). Aspectos moleculares del envejecimiento cutáneo. Dermatología Venezolana, 59(2).
This is a text version generated from the article. For the formatted version of record (with original tables & figures), download the PDF →