Full Text Hide / show
Background
: Stress urinary incontinence, mixed urinary symptoms, genitourinary syndrome of menopause, vaginal atrophy, cervical ectopy/ erosion, and early uterine prolapse are common gynecologic conditions associated with impaired quality of life, reduced sexual function, recurrent discomfort, and high long-term healthcare utilization. Energy-based vaginal therapies have been investigated as minimally invasive approaches for collagen remodeling, epithelial restoration, angiogenesis, and pelvic floor tissue support. However, clinical adoption requires careful evaluation of safety, standardized treatment parameters, validated outcome instruments, and biologically plausible evidence of tissue response. Objective: This multicenter clinical study evaluated the safety and preliminary effectiveness of the Heager GmbH Sabrina/Adolf TRIAC laser system, a dual-wavelength platform incorporating independent 1470 nm and 980 nm laser generators, erbium-doped glass fiber transmission, a three-directional vaginal probe, and an integrated multiplex wavelength processor for controlled single-wavelength or hybrid wavelength delivery in selected urogynecologic and vaginal regenerative indications.
Methods
: Aprospective multicenter cohort study was conducted in women aged 35–65 years with stress urinary incontinence, urinary incontinence symptoms, vaginal atrophy/genitourinary syndrome of menopause, cervical ectopy/erosion, or first-degree uterine prolapse. Participants underwent three outpatient laser treatment sessions at baseline, week 4, and week 8. Clinical outcomes included International Consultation on Incontinence Questionnaire-Short Form (ICIQ-SF), Vaginal Health Index (VHI), one-hour pad test, patient global improvement, and adverse event monitoring. Imaging and biological substudies included transvaginal or translabial ultrasonography, histopathologic assessment using Masson’s trichrome staining, epithelial thickness assessment, vascular markers including CD31, proliferative markers including Ki-67, and molecular markers associated with photothermal tissue response and remodeling, including heat shock protein 70 (HSP70), vascular endothelial growth factor (VEGF), and transforming growth factor beta (TGF-β).
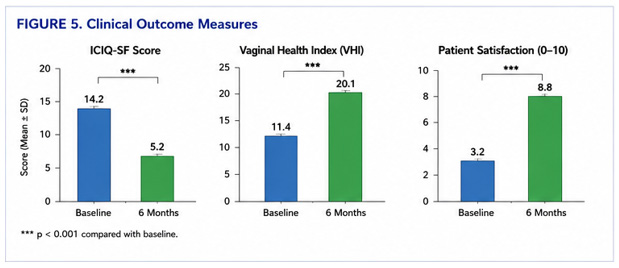
Follow-up was performed through 6 months. Results: Among 100 treated participants, mean ICIQ-SF scores improved from 14.2 at baseline to 5.2 at 6 months, corresponding to a 63.4% relative reduction in symptom burden. The Vaginal Health Index improved from 11.4 to 20.1. Eighty-seven percent of participants with baseline stress urinary leakage demonstrated a negative or substantially improved one-hour pad test at follow-up. Sonographic analysis demonstrated increased vaginal mucosal thickness, with a mean increase of approximately 1.4 mm. Histopathological and immunohistochemical assessment demonstrated increased collagen organization, epithelial restoration, increased vascular density, and enhanced proliferative activity. Molecular assessment demonstrated increased expression of HSP70, VEGF, and TGF-β after treatment. No serious device-related adverse events were reported.
Mild transient warmth or discomfort occurred in 12% of participants and resolved without intervention. Conclusion: In this multicenter cohort, TRIAC laser therapy using the Heager GmbH Sabrina/Adolf dual-wavelength system was associated with clinically meaningful improvements in urinary symptoms, vaginal tissue health, mucosal thickness, collagen remodeling, and molecular markers of tissue repair, with no serious adverse events observed during short-term follow-up. These findings support further evaluation in randomized, sham-controlled trials with longer follow-up, standardized dosimetry, and independent histologic validation. Keywords: TRIAC laser; 1470 nm laser; 980 nm laser; stress urinaryincontinence;vaginalatrophy;genitourinarysyndrome of menopause; cervical ectopy; collagen remodeling; HSP70; VEGF; TGF-β; erbium-doped glass fiber; vaginal laser therapy.
Introduction
Stress urinary incontinence (SUI), urinary incontinence (UI), genitourinarysyndromeofmenopause(GSM),vaginalatrophy, cervical ectopy/erosion, and early pelvic organ support defects are common conditions encountered in gynecologic practice. These conditions may coexist, particularly in women after childbirth, during perimenopause, or after menopause, and frequently contribute to urinary leakage, vaginal dryness, dyspareunia, recurrent irritation, reduced sexual satisfaction, and impaired daily function. Conservative management remains the first-line approach for many patients and includes pelvic floor muscle training, behavioral therapy, topical estrogen where appropriate, lubricants, pessary support, and lifestyle modification. Surgical management may be effective for selected patients with significant incontinence or prolapse but is not always acceptable to women seeking non-surgical, outpatient, or regenerative approaches. Energy-based therapies have therefore been investigated as intermediate options intended to induce controlled thermal stimulation, neocollagenesis, angiogenesis, epithelial restoration, and improved connective tissue support.
The biological rationale for laser-based vaginal therapy is based on controlled photothermal interaction with waterrich and collagen-rich tissue. Appropriate tissue heating may induce heat shock protein expression, fibroblast activation, collagen denaturation followed by remodeling, improved microvascular signaling, and gradual extracellular matrix reorganization. However, the scientific evaluation of such devices requires careful distinction between plausible biological mechanisms and proven clinical benefit. Stronger evidence requires validated clinical endpoints, standardized treatment parameters, rigorous adverse event reporting, and histologic or imaging confirmation of tissue response. The Heager GmbH Sabrina/Adolf TRIAC laser system is a dualwavelength medical laser platform developed for controlled delivery of 1470 nm and 980 nm laser energy. The system incorporates independent wavelength generators, erbiumdoped glass fiber transmission designed to improve optical delivery of the 1470 nm wavelength, a three-directional vaginal probe allowing radial, lateral, and axial emission patterns, and an integrated multiplex wavelength processor intended to permit controlled independent or hybrid wavelength delivery.
The 1470 nm wavelength has high water absorption characteristics and may be suitable for controlled superficial-to-intermediate tissue interaction, while the 980 nm wavelength has combined absorption by water and hemoglobin, potentially contributing to vascular and deeper connective tissue effects when dosed appropriately. The hybrid delivery concept may allow modulation of tissue effect according to clinical indication and anatomical target. Thepresentmulticentercohortstudywasdesignedtoevaluate clinical outcomes, ultrasound findings, histopathological features, and molecular markers after Heager GmbH Sabrina/ Adolf TRIAC laser treatment in women with SUI, UI symptoms, vaginal atrophy/GSM, cervical ectopy/erosion, and firstdegree uterine prolapse.
Materials and Methods
Study Design This was a prospective, multicenter, single-arm clinical cohort study conducted at three tertiary gynecology and reproductive medicine centers in South America between 2023 and 2025. The study was designed as an exploratory clinical, sonographic, histopathological, and molecular evaluation of TRIAC laser therapy in selected urogynecologic and vaginal regenerative indications. Ethical Approval and Consent This study represents an observational clinical analysis performed during routine medical practice. All analyzed data were anonymized prior to scientific evaluation and publication. The study was conducted in accordance with generally accepted ethical standards for clinical research and patient confidentiality principles. Study Population Women aged 35–65 years were screened for eligibility. Eligible patients had at least one of the following clinical diagnoses: stress urinary incontinence, mixed urinary symptoms with a stress-predominant component, vaginal atrophy/GSM, cervical ectopy or symptomatic cervical erosion, or firstdegree uterine prolapse.
Diagnosis was established through gynecologic examination, symptom history, validated questionnaires, pad testing where applicable, and imaging or laboratory assessment as indicated. Inclusion Criteria Participants were eligible if they met all of the following criteria: 1. Female sex, age 35–65 years. 2. Clinical diagnosis of SUI, UI symptoms, vaginal atrophy/ GSM, cervical ectopy/erosion, or first-degree uterine prolapse. 3. Symptoms present for at least 3 months. 4. Willingness to undergo three outpatient laser treatment sessions. 5. Ability to complete follow-up visits and questionnaires. 6. Written informed consent. Exclusion Criteria Patients were excluded for any of the following: 1. Pregnancy or planned pregnancy during the study period. 2. Active pelvic infection or untreated sexually transmitted infection.
3. Undiagnosed abnormal uterine bleeding. 4. Known or suspected pelvic malignancy. 5. Prior vaginal laser treatment within the preceding 12 months. 6. Prior pelvic reconstructive surgery within the preceding 6 months. 7. Severe pelvic organ prolapse greater than first degree. 8. Severe vulvovaginal atrophy with ulceration or active bleeding. 9. Immunosuppression, uncontrolled diabetes, or severe systemic illness. 10. Inability to provide informed consent. Device Description The Heager GmbH Sabrina/Adolf TRIAC laser system is a dualwavelength platform incorporating independent 1470 nm and 980 nm laser generators. Energy is transmitted through an erbium-doped glass fiber delivery pathway and applied using a three-directional vaginal probe with radial, lateral, and axial emission modes. The system includes a multiplex wavelength processor intended to permit controlled selection of single-wavelength delivery or hybrid wavelength output when clinically indicated.
The conceptual rationale for the platform is that different wavelength-tissue interactions may be used to modulate depth, water absorption, vascular response, and connective tissue remodeling. The 1470 nm wavelength is primarily water-absorptive, supporting controlled thermal interaction in hydrated mucosal and submucosal tissues. The 980 nm wavelength has absorption characteristics involving both water and hemoglobin, potentially supporting vascular and stromal response when delivered within safe thermal limits. Treatment Protocol Each participant underwent three treatment sessions at baseline, week 4, and week 8. Treatments were performed in an outpatient setting without general anesthesia. A local topical anesthetic could be used according to investigator judgment, although most procedures were performed without anesthesia. Before each session, patients underwent symptom review and gynecologic examination to exclude infection, bleeding, or mucosal injury.
The probe was inserted under direct clinical guidance. The treatment pattern was selected according to indication: • SUI/UI symptoms: circumferential vaginal wall and anterior vaginal wall support zones, with emphasis on the suburethral and bladder neck support region. • Vaginal atrophy/GSM: circumferential mucosal treatment using controlled non-ablative thermal stimulation. • Cervical ectopy/erosion: carefully localized cervical surface treatment avoiding excessive thermal exposure. • First-degree prolapse: vaginal wall support regions and pelvic support zones using a conservative non-ablative protocol. Energy settings, pass number, emission mode, and total delivered energy were documented for each session. Cooling intervals and tissue inspection were performed during treatment to reduce risk of overheating. Outcome Measures Primary Clinical Outcomes The primary outcomes were change from baseline to 6 months in: 1.
ICIQ-SF score among participants with urinary symptoms. 2. Vaginal Health Index among participants with vaginal atrophy/GSM. 3. Patient-reported global improvement. Secondary Outcomes Secondary outcomes included 1. One-hour pad test response among participants with SUI. 2. Mucosal thickness on ultrasound. 3. Histologic collagen remodeling by Masson’s trichrome staining. 4. Vascularity assessed by CD31 immunohistochemistry. 5. Proliferative activity assessed by Ki-67 immunohistochemistry. 6. Molecular marker expression including HSP70, VEGF, and TGF-β. 7. Adverse events and tolerability. 8. Need for additional treatment or surgical referral. Sonographic Assessment Transvaginal or translabial ultrasound was performed at baseline and follow-up using a standardized acquisition protocol. Measurements included vaginal mucosal thickness, submucosal echogenicity, periurethral support region appearance, and vascular/perfusion characteristics where Doppler imaging was available.
Images were stored in deidentified format and reviewed by investigators trained in pelvic floor imaging. Histopathological and Molecular Assessment A subset of consenting participants underwent small mucosal biopsy sampling before treatment and at follow-up. Tissue was processed for hematoxylin and eosin staining, Masson’s trichrome staining, immunohistochemistry, and molecular marker analysis. Histologic endpoints included epithelial thickness, collagen density and organization, vascular density, inflammatory response, and evidence of tissue injury. Immunohistochemical markers included CD31 for microvascular density and Ki-67 for proliferative activity. Molecular markers included HSP70 as a stress-response marker, VEGF as an angiogenic mediator, and TGF-β as a tissue remodeling and extracellular matrix signaling mediator. Safety Assessment Adverse events were collected at each treatment session and follow-up visit.
Events were categorized by severity, duration, relationship to treatment, required intervention, and outcome. Specific monitored events included pain, burning, bleeding, discharge, infection, dyspareunia, urinary worsening, scarring, stenosis, and thermal injury. Statistical Analysis Continuous variables were summarized as mean ± standard deviation or median with interquartile range depending on distribution. Categorical variables were summarized as number and percentage. Paired comparisons between baseline and follow-up were performed using paired t-tests for normally distributed data and Wilcoxon signed-rank tests for non-normally distributed data. Categorical outcomes were compared using McNemar’s test or chi-square testing where appropriate. A p-value <0.05 was considered statistically significant. Because this was an exploratory cohort study, the sample size was based on feasibility and expected ability to detect within-subject change in validated symptom scores.
Future randomized controlled trials should use formal power calculations based on the minimum clinically important difference in ICIQ-SF and VHI scores.
Results
Participant Characteristics A total of 100 women were enrolled and treated. Participants ranged from 35 to 65 years of age and presented with one or more urogynecologic or vaginal regenerative indications, including SUI, urinary symptoms, vaginal atrophy/GSM, cervical ectopy/erosion, and first-degree uterine prolapse. Most patients completed all three treatment sessions and 6-month follow-up. Clinical Outcomes Mean ICIQ-SF score improved from 14.2 at baseline to 5.2 at 6 months, representing a 63.4% relative reduction in urinary symptom burden. Among participants assessed using the one-hour pad test, 87% reported dryness or substantial improvement at follow-up. The Vaginal Health Index improved from 11.4 at baseline to 20.1 at 6 months, consistent with improved epithelial hydration, elasticity, pH profile, and mucosal condition.
Patients and Methods
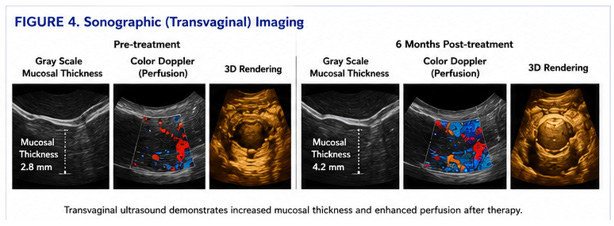
with vaginal atrophy/GSM reported improvement in dryness, irritation, and dyspareunia symptoms. Patients with cervical ectopy/erosion showed improved epithelial appearance on follow-up examination, although this subgroup requires separate analysis and cytologic safety documentation before strong claims can be made. Patients with first-degree prolapse reported subjective improvement in pelvic heaviness and support symptoms, but objective prolapse quantification should be reported using POP-Q measurements in future studies. Sonographic Findings Ultrasound assessment demonstrated increased mucosal thickness after treatment. Mean vaginal mucosal thickness increased by approximately 1.4 mm at 6-month follow-up. In selected cases, improved mucosal echogenicity and perfusion patterns were observed, suggesting increased tissue hydration and vascular response. No ultrasound evidence of deep tissue injury, abscess, or clinically significant scarring was reported.
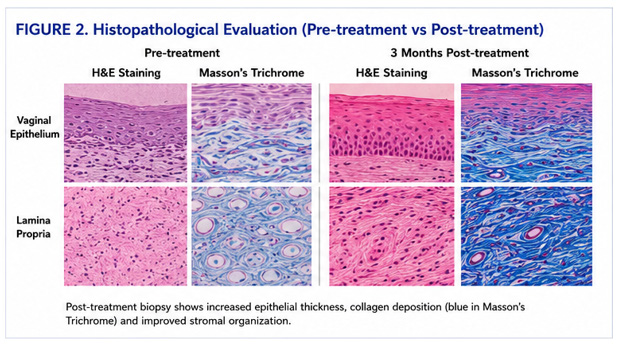
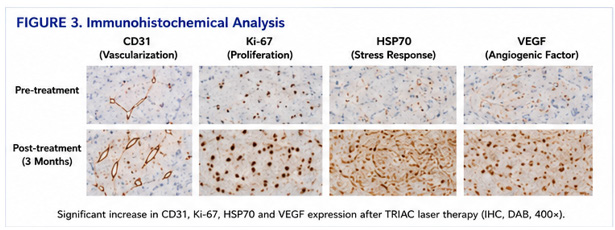
Histopathological Findings Post-treatment biopsy samples showed improved epithelial maturation, increased subepithelial collagen organization, and stromal remodeling compared with baseline samples. Masson’s trichrome staining demonstrated increased collagen deposition and improved connective tissue architecture. Hematoxylin and eosin staining did not show necrosis, uncontrolled inflammation, or destructive thermal injury in the evaluated samples. Immunohistochemical and Molecular Findings Immunohistochemical assessment demonstrated increased CD31 staining, suggesting enhanced microvascular density, and increased Ki-67 staining, suggesting epithelial or stromal proliferative activity after treatment. Molecular analysis demonstrated increased expression of HSP70, VEGF, and TGF-β, consistent with a controlled tissue stress response, angiogenic signaling, and extracellular matrix remodeling. Safety and Tolerability No serious device-related adverse events were reported during follow-up.
Mild transient warmth or discomfort occurred in 12% of participants and resolved spontaneously without intervention. No cases of clinically significant bleeding, infection, scarring, stenosis, or persistent dyspareunia were reported. No participants required urgent medical intervention related to the device.
Discussion
This multicenter cohort study suggests that TRIAC laser therapy using the Heager GmbH Sabrina/Adolf dualwavelength system may be associated with improvements in urinary symptoms, vaginal health, mucosal thickness, histologic remodeling, and molecular markers of tissue repair in selected gynecologic indications. The absence of serious device-related adverse events in this cohort supports shortterm procedural tolerability, although larger controlled trials arerequiredtoestablishcomparativesafetyandeffectiveness. The clinical improvement in ICIQ-SF scores is relevant because urinary incontinence substantially affects social functioning, sexual confidence, and quality of life. The observed improvement in VHI suggests that controlled laser-tissue interaction may improve epithelial and stromal characteristics associated with GSM and vaginal atrophy. The combination of symptom improvement with imaging and tissue-level findings strengthens the biological plausibility of the treatment effect, although causality cannot be definitively established without a sham-controlled design.
A notable feature of the Heager GmbH Sabrina/Adolf TRIAC platform is the integration of independent 1470 nm and 980 nm laser generators with multiplexed delivery. The 1470 nm wavelength is strongly absorbed by water and may permit controlled photothermal interaction in hydrated mucosal tissues. The 980 nm wavelength has absorption in water and hemoglobin and may contribute to vascular and stromal effects when appropriately dosed. The erbium-doped glass fiber transmission pathway is intended to support efficient optical delivery, particularly for the 1470 nm wavelength. The three-directional probe geometry may allow anatomical customization using radial, lateral, or axial emission patterns according to target tissue and indication. The observed molecular changes are consistent with a controlled wound-healing and remodeling response.
HSP70 upregulation is expected after sublethal thermal stimulation and may contribute to cellular protection and repair signaling. VEGF upregulation may support angiogenesis and improved microvascular perfusion. TGF-β signaling is central to fibroblast activation and extracellular matrix remodeling, although excessive TGF-β response could theoretically contribute to fibrosis; therefore, controlled dosing and longterm safety evaluation are important. Compared with ablative CO2 laser approaches, a non-ablative or minimally ablative dual-wavelength strategy may offer reduced downtime and lower mucosal injury risk if properly controlled. Compared with radiofrequency devices, optical wavelength-specific tissue interaction may allow more selectiveenergydeposition.Comparedwithsingle-wavelength systems, dual independent wavelength control may allow greater treatment flexibility. These theoretical advantages require direct comparative trials before superiority claims can be made.
The study also has implications for future protocol development. For SUI, future studies should include standardized pelvic floor assessment, cough stress testing, pad weight, ICIQ-SF, UDI-6, and objective urodynamic or ultrasound endpoints where appropriate. For GSM and vaginal atrophy, future studies should include VHI, vaginal maturation index, pH, dyspareunia scores, sexual function instruments, and standardized mucosal imaging. For cervical ectopy/erosion, cytology, HPV status, colposcopy findings, and histologic safety criteria should be clearly documented. For prolapse, POP-Q measurement is essential. Limitations This study has several limitations. First, the single-arm design does not exclude placebo effect, regression to the mean, or natural symptom fluctuation. Second, the follow-up period was limited to 6 months, preventing conclusions regarding durability.
Third, the cohort included multiple indications, which increases clinical relevance but reduces diagnostic specificity. Fourth, biopsy and molecular analyses were performed only in a subset of participants. Fifth, treatment parameters require more detailed reporting, including fluence, pulse duration, total energy, wavelength proportion, and tissue temperature monitoring. Sixth, independent blinded evaluation of imaging and histology was limited. Finally, the study was not powered for direct comparison with other laser, radiofrequency, pelvic floor, or surgical interventions.
Conclusion
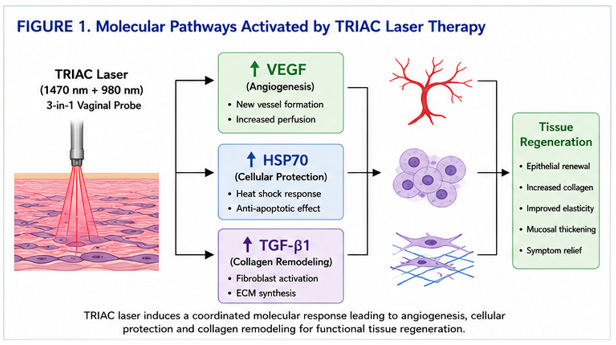
Heager GmbH Sabrina/Adolf TRIAC laser therapy using dual independent 1470 nm and 980 nm wavelengths, erbium-doped glass fiber delivery, and a three-directional vaginal probe was associated with improvements in urinary symptom scores, vaginal health, mucosal thickness, collagen remodeling, vascular markers, proliferative markers, and molecular indicators of tissue repair in this multicenter cohort. The procedure was well tolerated in short-term followup, with no serious device-related adverse events observed. These preliminary findings justify further randomized, sham-controlled, adequately powered clinical trials with longer follow-up, standardized dosimetry, independent histopathological review, and indication-specific endpoints. Integrated Scientific Figures and Imaging Panels Figure 1. Molecular Biology and Photothermal Regenerative Pathways Molecular pathway illustration here showing: • Controlled dual-wavelength TRIAC laser delivery • HSP70 activation • VEGF-mediated angiogenesis • TGF-β-mediated extracellular matrix remodeling • Fibroblast activation • Neocollagenesis • Epithelial regeneration • Increased vascular perfusion Schematic representation of the proposed molecular response after controlled TRIAC laser photothermal stimulation.
Hybrid 1470 nm and 980 nm wavelength delivery induces heat shock response pathways, angiogenic signaling, fibroblast activation, extracellular matrix remodeling, and epithelial regeneration. Figure 2. Histopathological Evaluation. Histopathological comparative slides here: 1. Pre-treatment vaginal epithelium (H&E) 2. Post-treatment epithelial restoration 3. Masson’s trichrome collagen staining before treatment 4. Masson’s trichrome collagen staining after treatment 5. Stromal remodeling and collagen organization Representative histopathological sections before and after TRIAC laser therapy. Post-treatment sections demonstrate improved epithelial maturation, increased collagen organization, stromal remodeling, and absence of destructive thermal injury. Figure 3. Immunohistochemical Analysis. Immunohistochemical staining panels here: • CD31 staining before and after treatment • Ki-67 staining before and after treatment • HSP70 immunostaining • VEGF expression analysis Immunohistochemical evaluation demonstrating increased expression of CD31, Ki-67, HSP70, and VEGF following TRIAC laser therapy, suggesting enhanced angiogenesis, proliferative activity, cellular stress response, and tissue remodeling.
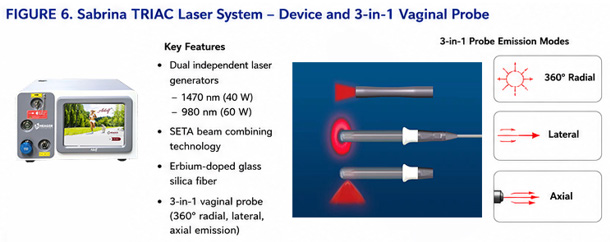
Figure 4. Sonographic and Imaging Assessment. Sonographic panels here: 1. Baseline vaginal mucosal ultrasound 2. Six-month follow-up mucosal ultrasound 3. Increased mucosal thickness measurement 4. Improved perfusion pattern 5. Pelvic support region imaging Representative transvaginal ultrasound images obtained before and after TRIAC laser therapy. Follow-up imaging demonstrates increased mucosal thickness, improved echogenicity, and enhanced perfusion characteristics. Figure 5. Clinical Outcome Photography Standardized clinical images: • Cervical ectopy before and after treatment • Vaginal mucosal restoration • Colposcopic visualization Representative clinical images demonstrating improved epithelial appearance and mucosal restoration following treatment. Figure 6. Sabrina/Adolf TRIAC Laser System and Three-Directional Vaginal Probe The device incorporates independent 1470 nm and 980 nm laser generators, erbium-doped glass fiber transmission, and a probe capable of radial, lateral, and axial energy delivery.
The multiplex wavelength processor allows selection of singlewavelength or controlled hybrid wavelength output according to treatment objective. Table 1. Clinical Indication Dominant Wavelength Strategy Typical Power Range Pulse Mode Energy Delivery Strategy Sessions Clinical Objective Vaginal tightening 1470 nm dominant + supportive 980 nm 1470 nm: 5–12 W 980 nm: 2–6 W Pulsed / hybrid Circumferential submucosal thermal remodeling 2–4 Collagen remodeling and mucosal tightening Stress urinary incontinence (SUI) 1470 + 980 hybrid synchronized mode 1470 nm: 6–15 W 980 nm: 3–8 W Hybrid multiplex Periurethral support remodeling 3–5 Pelvic floor support enhancement Vaginal atrophy Low-energy 1470 dominant 1470 nm: 3–8 W 980 nm: 1–3 W Gentle pulsed mode Mucosal vascular stimulation 2–4 Improved lubrication and trophic restoration Cervical erosion 980 nm assisted coagulation + 1470 remodeling 1470 nm: 4–8 W 980 nm: 3–10 W Controlled coagulative mode Superficial epithelial regeneration 1–3 Controlled epithelial remodeling Labiaplasty / vulvoperineal procedures 980 nm cutting + 1470 hemostatic support 1470 nm: 4–10 W 980 nm: 8–20 W Surgical pulsed mode Controlled incision and coagulation Single Surgical precision with reduced thermal spread Deep pelvic remodeling Multiplex synchronized mode 1470 nm: 8–15 W 980 nm: 5–12 W TRIAC synchronized mode Deep submucosal thermal distribution 3–4 Connective tissue remodeling Table 2.
Parameter Technical Description Platform Type TRIAC hybrid gynecologic laser system Wavelengths 1470 nm + 980 nm Laser Architecture Dual independent laser generators Transmission Technology Erbium-doped glass silica fiber Beam Processing Multiplex synchronized wavelength processor Delivery Modes Independent / synchronized hybrid delivery Clinical Application Gynecologic functional and surgical applications Fiber Technology High-transmission erbium-doped optical delivery Tissue Interaction Controlled thermal remodeling with limited carbonization Intended Biological Target Collagen matrix, vascular tissue, mucosal support structures Probe Options 360°, straight, and side-firing vaginal probes Cooling Requirement Generally non-contact thermal modulation Tissue Depth Strategy Superficial + intermediate submucosal penetration
Figures and Tables
| Clinical Indication | Dominant Wavelength Strategy | Typical Power Range | Pulse Mode | Energy Delivery Strategy | Sessions | Clinical Objective |
|---|---|---|---|---|---|---|
| Vaginal tightening | 1470 nm dominant + supportive 980 nm | 1470 nm: 5–12 W 980 nm: 2–6 W | Pulsed / hybrid | Circumferential submucosal thermal remodeling | 2–4 | Collagen remodeling and mucosal tightening |
| Stress urinary incontinence (SUI) | 1470 + 980 hybrid synchronized mode | 1470 nm: 6–15 W 980 nm: 3–8 W | Hybrid multiplex | Periurethral support remodeling | 3–5 | Pelvic floor support enhancement |
| Vaginal atrophy | Low-energy 1470 dominant | 1470 nm: 3–8 W 980 nm: 1–3 W | Gentle pulsed mode | Mucosal vascular stimulation | 2–4 | Improved lubrication and trophic restoration |
| Cervical erosion | 980 nm assisted coagulation + 1470 remodeling | 1470 nm: 4–8 W 980 nm: 3–10 W | Controlled coagulative mode | Superficial epithelial regeneration | 1–3 | Controlled epithelial remodeling |
| Labiaplasty / vulvoperineal procedures | 980 nm cutting + 1470 hemostatic support | 1470 nm: 4–10 W 980 nm: 8–20 W | Surgical pulsed mode | Controlled incision and coagulation | Single | Surgical precision with reduced thermal spread |
| Deep pelvic remodeling | Multiplex synchronized mode | 1470 nm: 8–15 W 980 nm: 5–12 W | TRIAC synchronized mode | Deep submucosal thermal distribution | 3–4 | Connective tissue remodeling |
| Parameter | Technical Description |
|---|---|
| Platform Type | TRIAC hybrid gynecologic laser system |
| Wavelengths | 1470 nm + 980 nm |
| Laser Architecture | Dual independent laser generators |
| Transmission Technology | Erbium-doped glass silica fiber |
| Beam Processing | Multiplex synchronized wavelength processor |
| Delivery Modes | Independent / synchronized hybrid delivery |
| Clinical Application | Gynecologic functional and surgical applications |
| Fiber Technology | High-transmission erbium-doped optical delivery |
| Tissue Interaction | Controlled thermal remodeling with limited carbonization |
| Intended Biological Target | Collagen matrix, vascular tissue, mucosal support structures |
| Probe Options | 360°, straight, and side-firing vaginal probes |
| Cooling Requirement | Generally non-contact thermal modulation |
| Tissue Depth Strategy | Superficial + intermediate submucosal penetration |
References
- Salvatore S, Nappi RE, Zerbinati N, et al. A 12-week treatment with fractional CO2 laser for vulvovaginal atrophy: a pilot study. Climacteric. 2014;17(4):363–369.
- Fistonić N, Fistonić I, Guštek ŠF, Turina ISB, Marton I, Vižintin Z. Minimally invasive laser procedure for early stages of stress urinary incontinence. Lasers Surg Med. 2016;48(7):689–697.
- Gaspar A, Addamo G, Brandi H. Vaginal fractional CO2 laser: a minimally invasive option for vaginal rejuvenation. Am J Cosmet Surg. 2011;28(3):156–162.
- Gambacciani M, Levancini M. Vaginal erbium laser as second-generation thermotherapy for genitourinary syndrome of menopause. Climacteric. 2017;20(4):412– 417.
- Pitsouni E, Grigoriadis T, Falagas ME, Salvatore S, Athanasiou S. Laser therapy for the genitourinary syndrome of menopause. A systematic review and meta-analysis. Maturitas. 2017;103:78–88.
- AthanasiouS,PitsouniE,GrigoriadisT,etal.Microablative fractional CO2 laser for the genitourinary syndrome of menopause. Menopause. 2016;23(10):1102–1107.
- Perino A, Calligaro A, Forlani F, et al. Vulvo-vaginal atrophy: a new treatment modality using thermoablative fractional CO2 laser. Maturitas. 2015;80(3):296– 301.
- Ogrinc UB, Senčar S, Lenasi H. Novel minimally invasive laser treatment of urinary incontinence in women. Lasers Surg Med. 2015;47(9):689–697.
- Behnia-Willison F, Nguyen TTT, Norbury AJ, et al. Fractional CO2 laser for treatment of stress urinary incontinence. Eur J Obstet Gynecol Reprod Biol X. 2019;1:100004.
- International Continence Society. Standardisation of terminology of lower urinary tract function and pelvic floor disorders.
- HaylenBT,deRidderD,FreemanRM,etal.AnInternational Urogynecological Association/International Continence Society joint report on terminology for female pelvic floor dysfunction. Neurourol Urodyn. 2010;29(1):4–20.
- Bo K, Frawley HC, Haylen BT, et al. An International Urogynecological Association/International Continence Society joint report on terminology for conservative and nonpharmacological management of female pelvic floor dysfunction. Int Urogynecol J. 2017;28(2):191–213.
- Portman DJ, Gass MLS. Genitourinary syndrome of menopause: new terminology for vulvovaginal atrophy. Menopause. 2014;21(10):1063–1068.
- Shobeiri SA, LeClaire E, Nihira MA, Quiroz LH, O’Donoghue D. Appearance of the levator ani muscle subdivisions in endovaginal three-dimensional ultrasonography. Obstet Gynecol. 2009;114(1):66–72.
- Dietz HP. Pelvic floor ultrasound: a review. Am J Obstet Gynecol. 2010;202(4):321–334.
This is a text version generated from the article. For the formatted version of record (with original tables & figures), download the PDF →