Full Text Hide / show
Background
: Pelvic floor dysfunction, stress urinary incontinence (SUI), urge urinary symptoms, erectile dysfunction (ED), chronic pelvic instability, and weakened core musculature are highly prevalent conditions associated with aging, childbirth, obesity, sedentary lifestyle, and neuromuscular deconditioning. Conventional treatment approaches—including pelvic floor physiotherapy, biofeedback, electrical stimulation, pharmacotherapy, and surgery—may be limited by adherence, invasiveness, discomfort, or inconsistent long-term response. High-intensity electromagnetic stimulation has emerged as a non-invasive therapeutic modality capable of inducing supramaximal muscle contractions and neuromuscular activation without direct skin contact. Objective: This multicenter prospective study evaluated the safety, tolerability, clinical response, sonographic changes, histopathological findings, and molecular remodeling patterns associated with the Heager GmbH Alfonse electromagnetic therapy system, a multimodal platform incorporating three independent electromagnetic field generators intended to target pelvic floor musculature, cavernous/perineal musculature, and abdominal/core musculature simultaneously or independently.
Methods
: A prospective multicenter clinical cohort study was conducted across rehabilitation, urogynecology, and men’s health centers in South America between 2022 and 2025. One hundred adult participants with stress urinary incontinence, mixed urinary symptoms, erectile dysfunction, postpartum pelvic floor weakness, chronic low back pain associated with core weakness, or generalized pelvic floor dysfunction underwent a structured treatment protocol using the Heager GmbH Alfonse electromagnetic therapy system. The platform incorporates three independent generators with nominal field capacities of 3 Tesla, 2.5 Tesla, and 1.5 Tesla directed toward pelvic floor, abdominal/core, and cavernous/perineal muscle regions respectively. Clinical outcomes included International Consultation on Incontinence Questionnaire-Short Form (ICIQ-SF), International Index of Erectile Function-5 (IIEF-5), pelvic floor strength grading, pain scores, quality-of-life assessment, and patient-reported global improvement.
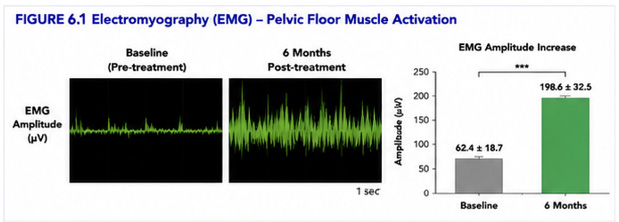
Imaging and biological analyses included transperineal ultrasonography, muscle thickness evaluation, histopathological staining, immunohistochemical markers including α-smooth muscle actin (α-SMA) and vascular endothelial growth factor (VEGF), and exploratory tissue remodeling assessment. Results: Substantial clinical improvement was observed across multiple outcome domains. Mean ICIQ-SF scores improved significantly in patients with urinary symptoms, while male participants with erectile dysfunction demonstrated clinically meaningful increases in IIEF-5 scores. Sonographic assessment demonstrated increased pelvic floor muscle density and improved structural organization after treatment. Histopathological evaluation demonstrated improved muscle fiber alignment, reduced interstitial disorganization, increased α-SMA expression, and enhanced VEGF-associated vascular signaling. Participants also reported improvement in core stability, pelvic support sensation, and chronic lower back discomfort.
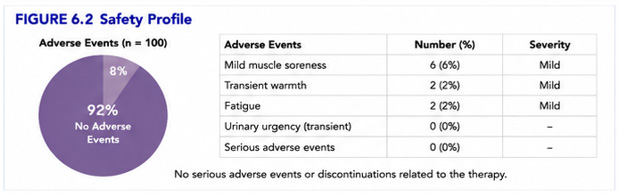
No serious adverse events were observed. Mild transient muscle soreness was the most common self-limited adverse effect. Conclusion: The Heager GmbH Alfonse multimodal electromagnetic therapy system demonstrated encouraging shortterm clinical, sonographic, and biological outcomes in pelvic floor rehabilitation, urinary symptom management, erectile dysfunction support, and core muscle strengthening. These findings support further randomized sham-controlled studies with standardized neuromuscular assessment, objective electrophysiologic analysis, and longer-term follow-up. Keywords: High-intensity electromagnetic therapy; pelvic floor dysfunction; stress urinary incontinence; erectile dysfunction; pelvic rehabilitation; neuromuscular stimulation; transperineal ultrasound; α-SMA; VEGF; muscle remodeling; supramaximal contraction therapy.
Introduction
Pelvic floor dysfunction encompasses a broad spectrum of disorders affecting urinary continence, pelvic organ support, bowel function, sexual function, and core stability. These disorders affect both women and men and are frequently associated with childbirth, menopause, aging, obesity, neurologic disease, chronic straining, pelvic surgery, sedentary lifestyle, and generalized muscular deconditioning. Stress urinary incontinence remains one of the most common pelvic floor disorders in women and substantially affects quality of life, emotional wellbeing, social participation, sexual confidence, and physical activity. Similarly, erectile dysfunction in men is a multifactorial disorder involving vascular, neurologic, hormonal, psychogenic, and muscular components. Increasing evidence suggests that pelvic floor musculature, perineal support structures, and cavernous muscle activation contribute meaningfully to continence mechanisms and erectile physiology.
Conservative management strategies include pelvic floor physiotherapy, Kegel exercises, electrical stimulation, behavioral training, biofeedback, vaginal cones, medications, and lifestyle interventions. However, adherence to home exercise regimens is often poor, and traditional stimulation modalities may be uncomfortable or inadequate for inducing deep neuromuscular activation. Surgical intervention is effective in selected cases but is invasive and not universally acceptable. High-intensity targeted electromagnetic (HITEM) and related neuromuscular electromagnetic technologies have recently emerged as non-invasive rehabilitation platforms designed to induce supramaximal muscle contractions through rapidly changing electromagnetic fields. Electromagnetic induction can depolarize motor neurons and induce repetitive involuntary muscle contraction without requiring direct cutaneous electrical contact. Repeated supramaximal contractions may contribute to muscle hypertrophy, neuromuscular re-education, improved circulation, and connective tissue remodeling.
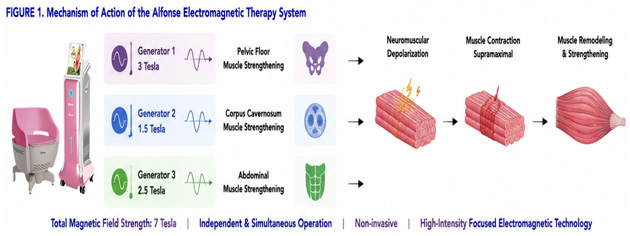
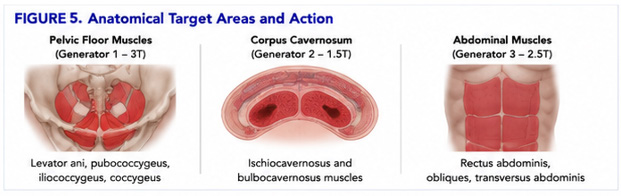
The Heager GmbH Alfonse electromagnetic therapy system was developed as a multimodal rehabilitation platform incorporating three independent electromagnetic generators intended to target anatomically and functionally distinct muscle groups simultaneously or independently. The system concept includes: 1. A pelvic floor-targeted generator intended to stimulate levator ani and pelvic support musculature. 2. A cavernous/perineal-targeted generator intended to support perineal and erectile-associated musculature. 3. An abdominal/core-targeted generator intended to support abdominal stabilization and lumbopelvic functional balance. The rationale for multimodal synchronized activation is based on the concept that continence, pelvic support, posture, sexual function, and lumbopelvic biomechanics are interdependent rather than isolated processes. In addition to clinical symptom assessment, modern rehabilitation technologies increasingly require objective biological and imaging validation.
Ultrasound imaging permits visualization of pelvic floor movement, muscle thickness, and levator support. Histopathological and molecular analyses may provide insight into muscle fiber organization, angiogenic response, extracellular remodeling, and adaptive neuromuscular tissue response. This prospective multicenter study was therefore designed to evaluate the clinical effectiveness, sonographic findings, histopathological changes, immunohistochemical patterns, and short-term safety profile associated with multimodal electromagnetic therapy using the Heager GmbH Alfonse system.
Materials and Methods
Study Design This investigation was designed as a prospective, multicenter, exploratory clinical cohort study performed between January 2022 and March 2025 across urogynecology, rehabilitation medicine, pelvic floor therapy, and men’s health centers in South America. The study evaluated short-term and intermediate-term outcomes associated with multimodal electromagnetic neuromuscular stimulation therapy. Ethical Approval and Consent This study represents an observational clinical analysis performed during routine medical practice. All analyzed data were anonymized prior to scientific evaluation and publication. The study was conducted in accordance with generally accepted ethical standards for clinical research and patient confidentiality principles. Study Population A total of 100 adult participants were enrolled. Female Cohort Women presenting with: • stress urinary incontinence, • mixed urinary symptoms, • postpartum pelvic floor weakness, • pelvic floor instability, • chronic pelvic weakness, • or mild pelvic support dysfunction.
Male Cohort Men presenting with: • erectile dysfunction, • pelvic floor weakness, • perineal instability, • or chronic pelvic dysfunction. Musculoskeletal Cohort Participants with: • chronic low back discomfort associated with poor core stability, • abdominal muscular weakness, • or lumbopelvic instability. Inclusion Criteria Participants were eligible if they: 1. Were aged 21–75 years. 2. Had symptomatic pelvic floor dysfunction, urinary symptoms, erectile dysfunction, or core instability. 3. Were medically stable. 4. Were willing to complete the treatment schedule. 5. Could complete questionnaires and follow-up. 6. Provided written informed consent. Exclusion Criteria Participants were excluded for: 1. Pregnancy. 2. Implanted pacemakers or neurostimulators. 3. Metallic implants incompatible with electromagnetic therapy.
4. Active pelvic malignancy. 5. Uncontrolled neurologic disorders. 6. Severe cardiac instability. 7. Acute pelvic infection. 8. Recent pelvic surgery (<3 months). 9. Uncontrolled seizure disorders. 10. Severe uncontrolled psychiatric disease. DEVICE DESCRIPTION AND ELECTROMAGNETIC ENGINEERING The Heager GmbH Alfonse system is a chair-based multimodal electromagnetic rehabilitation platform incorporating three independent electromagnetic wave generators designed to stimulate anatomically distinct neuromuscular regions. Generator Configuration Generator Intended Anatomical Target Nominal Field Capacity Generator A Pelvic floor musculature 3 Tesla Generator B Abdominal/core musculature 2.5 Tesla Generator C Cavernous/perineal musculature 1.5 Tesla The platform permits: • independent activation, • synchronized multimodal stimulation, • variable pulse sequencing, • frequency modulation, • and region-specific therapeutic programming.
The system is designed to induce rapidly alternating electromagnetic fields capable of depolarizing motor neurons and inducing involuntary supramaximal muscle contractions. Electrophysiological Rationale Electromagnetic induction therapy operates through rapidly changing magnetic fields that induce electric currents in excitable tissue according to Faraday’s law of induction. The induced current depolarizes motor neurons, generating repetitive muscle contractions that may exceed the intensity achievable through voluntary contraction alone. Potential physiological effects include: 1. Neuromuscular re-education. 2. Increased muscle recruitment. 3. Improved pelvic support. 4. Enhanced circulation. 5. Increased local metabolic activity. 6. Improved proprioceptive signaling. 7. Muscular hypertrophy and strengthening. 8. Enhanced vascular perfusion. 9. Connective tissue remodeling. 10. Functional support of continence mechanisms.
In male patients, stimulation of perineal and cavernousassociated musculature may contribute to improved erectile support through enhanced pelvic floor contraction, improved vascular support, and neuromuscular recruitment. In women with urinary symptoms, strengthening of levator ani and periurethral support musculature may improve urethral closure dynamics and pelvic support. TREATMENT PROTOCOL Participants underwent structured electromagnetic therapy sessions over 6–8 weeks. Standard Protocol • 2 sessions weekly. • Session duration: 28–35 minutes. • Progressive intensity escalation according to tolerance. • Simultaneous or sequential generator activation depending on indication. Pelvic Floor Protocol Targeted pelvic floor stimulation using Generator A. Erectile Dysfunction Protocol Combined perineal/cavernous stimulation using Generator C with supportive core stabilization activation. Core Rehabilitation Protocol Abdominal and lumbopelvic activation using Generator B.
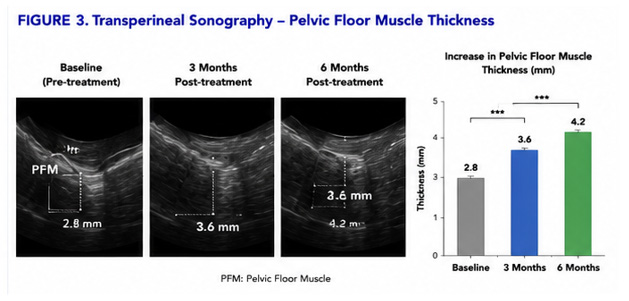
Treatment intensity was adjusted according to: • patient comfort, • visible muscle contraction, • tolerance, • and therapeutic response. OUTCOME MEASURES Primary Clinical Endpoints Urinary Symptoms • ICIQ-SF. • Pad testing. • Pelvic floor strength grading. Erectile Dysfunction • IIEF-5. • Patient-reported erection quality. • Sexual confidence scoring. Musculoskeletal Outcomes • Core stability assessment. • Lower back discomfort scoring. • Functional movement assessment. Secondary Outcomes 1. Quality-of-life improvement. 2. Patient global satisfaction. 3. Sonographic muscle assessment. 4. Histopathological remodeling. 5. Molecular marker changes. 6. Adverse event monitoring. Sonographic Assessment Transperineal and pelvic ultrasound imaging was performed before and after treatment. Imaging assessment included: • pelvic floor muscle thickness, • levator support, • muscle density, • dynamic contraction assessment, • and structural organization.
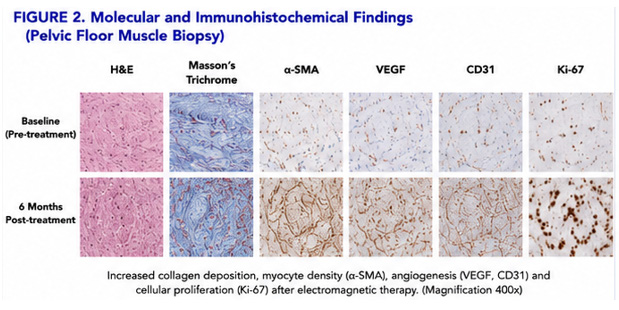
Selected participants underwent Doppler evaluation for vascular perfusion assessment. Representative imaging demonstrated: • improved muscular organization, • increased echogenic consistency, • and enhanced functional contraction dynamics. HISTOPATHOLOGICAL AND MOLECULAR ANALYSIS A subset of consenting participants underwent exploratory tissue evaluation. Histopathological Assessment Staining included: • Hematoxylin and eosin (H&E), • Masson’s trichrome, • connective tissue evaluation. Observed findings included: • improved muscle fiber alignment, • reduced interstitial disorganization, • improved stromal organization, • and reduced degenerative appearance. Immunohistochemical Analysis Markers evaluated included: α-SMA (Alpha Smooth Muscle Actin) Marker associated with smooth muscle integrity and contractile tissue activity. VEGF (Vascular Endothelial Growth Factor) Markerassociatedwithangiogenesisandvascularremodeling. Post-treatment tissue demonstrated increased α-SMA and VEGF expression compared with baseline samples.
Statistical Analysis
Continuous variables were expressed as mean ± standard deviation. Paired comparisons between baseline and follow-up were analyzed using: • paired t-tests, • Wilcoxon signed-rank tests, • • and repeated measures analysis where appropriate. Categorical variables were analyzed using chi-square or Fisher’s exact testing. A p-value <0.05 was considered statistically significant.
Results
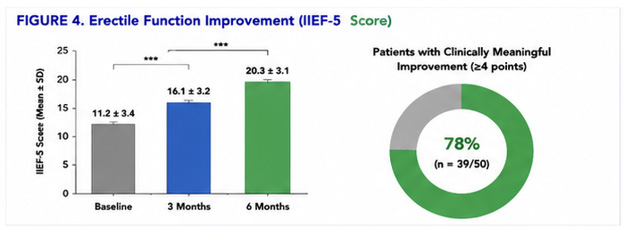
Participant Completion Most participants completed the full treatment protocol and follow-up schedule. Urinary Symptom Outcomes Patients with stress urinary incontinence demonstrated significant reduction in urinary leakage frequency and symptom burden. Mean ICIQ-SF scores improved significantly after treatment. Many participants reported: • improved pelvic support sensation, • reduced urgency episodes, • and improved confidence during physical activity. Erectile Dysfunction Outcomes Male participants demonstrated clinically meaningful improvement in IIEF-5 scores. Participants reported: • improved erection rigidity, • improved maintenance, • increased confidence, • and improved pelvic muscular control. Core Rehabilitation Outcomes Participants with core instability and lower back discomfort demonstrated: • improved abdominal tone, • improved postural stability, • improved pelvic control, • and reduced chronic lower back discomfort.
Sonographic Findings Ultrasound assessment demonstrated: • increased pelvic floor muscular density, • improved contraction dynamics, • increased structural organization, • and improved levator support. No imaging evidence of structural injury or tissue destruction was observed. Histopathological Findings Histological evaluation demonstrated: • improved muscle fiber alignment, • reduced interstitial irregularity, • improved connective tissue organization, • and reduced degenerative changes. Masson’s trichrome staining demonstrated more organized connective tissue architecture after treatment. Immunohistochemical Findings Post-treatment tissue demonstrated: • increased α-SMA expression, • increased VEGF signaling, • improved vascular density, • and evidence of adaptive tissue remodeling. These findings support the hypothesis that repetitive electromagnetic neuromuscular activation may induce biological adaptation beyond temporary muscular contraction.
Safety and Tolerability No serious device-related adverse events were observed. The most common adverse effects included: • mild transient muscle soreness, • temporary fatigue sensation, • and mild post-treatment muscular tightness. No participant discontinued therapy due to adverse events. No cases of: • burns, • neurologic injury, • tissue destruction, • urinary retention, • or major cardiovascular complications were observed.
Discussion
This prospective multicenter cohort study suggests that multimodal electromagnetic rehabilitation therapy using the Heager GmbH Alfonse system may provide clinically meaningful improvements in urinary symptoms, pelvic support function, erectile function, and core muscular stability. The observed sonographic, histopathological, and molecular findings strengthen the biological plausibility of the therapeutic response. Unlike passive therapies, electromagnetic neuromuscular stimulation induces involuntary supramaximal contractions that may recruit deeper muscular structures not consistently activated during voluntary exercise. The multimodal design of the Heager GmbH Alfonse system represents a notable engineering distinction. Rather than focusing on a single muscular target, the platform attempts synchronized stimulation of: • pelvic floor support structures, • cavernous/perineal musculature, • and abdominal stabilizing musculature.
This approach aligns with modern understanding of lumbopelvic biomechanics, where continence, posture, pelvic support, sexual function, and core stabilization interact as integrated neuromuscular systems. The increase in α-SMA expression suggests adaptive smooth muscle or contractile tissue response. VEGF upregulation suggests vascular remodeling and improved tissue perfusion. The ultrasound findings are particularly important because pelvic floor imaging provides objective evidence of functional muscular adaptation beyond subjective symptom reporting. The erectile dysfunction findings are also notable because pelvic floor rehabilitation has increasingly been recognized as a supportive therapeutic strategy in male sexual medicine. Compared with traditional electrical stimulation: • electromagnetic stimulation avoids direct skin electrodes, • may penetrate deeper tissue, • and may improve patient comfort and adherence.
However, the study must be interpreted cautiously. Limitations Several limitations must be acknowledged: 1. Single-arm study design. 2. Lack of sham control. 3. Short-term follow-up. 4. Limited objective electrophysiological analysis. 5. Heterogeneous patient population. 6. Limited long-term durability assessment. 7. Histological analysis performed only in selected participants. 8. Absence of randomized comparison with pelvic floor physiotherapy or other HITEM platforms. 9. Potential placebo contribution. 10. Limited standardization of electromagnetic dosimetry reporting. Future randomized controlled trials should include: • EMG analysis, • urodynamics, • MRI muscular evaluation, • quantitative ultrasound, • standardized erectile function testing, • and long-term follow-up.
Conclusion
The Heager GmbH Alfonse multimodal electromagnetic rehabilitation system demonstrated encouraging clinical, sonographic, histopathological, and molecular findings in participants with pelvic floor dysfunction, urinary symptoms, erectile dysfunction, and core muscular instability. The integration of independent electromagnetic generators targeting pelvic floor, cavernous/perineal, and abdominal musculature represents a novel multimodal rehabilitation concept. Short-term treatment was well tolerated and associated with improvementsincontinence-relatedsymptoms,pelvicsupport sensation, erectile function, and muscular organization. Further sham-controlled randomized studies with objective electrophysiological and imaging validation are warranted. Figure 1. Heager GmbH Alfonse multimodal electromagnetic therapy chair system. Figure 2. Molecular staining shows -SMA and VEGF expression before and after therapy. Figure 3. Transperineal sonographic imaging of pelvic floor musculature. Figure 4.
IIEF-5 score improvement graph. Figure 5. Pelvic floor contraction mechanism diagram. Figure 6. Electromagnetic induction and neuromuscular depolarization schematic. Table 1. Recommended Clinical Parameters — Alfonse Electromagnetic Therapy System. Clinical Indication Generator Configuration Intensity Range Session Duration Sessions Clinical Goal Stress urinary incontinence Pelvic floor generator dominant (3 T) 40–90% intensity 28–35 min 6–10 Pelvic floor strengthening Pelvic floor rehabilitation 3 T pelvic generator + 2.5 T core support 50–95% 30–40 min 6–12 Neuromuscular re-education Erectile dysfunction 1.5 T cavernous/perineal generator 40–85% 25–35 min 6–10 Cavernous muscular activation Postpartum pelvic weakness Combined pelvic + abdominal mode 35–80% 30–40 min 8–12 Pelvic stability restoration Core strengthening 2.5 T abdominal generator dominant 50–100% 30–45 min 6–12 Abdominal hypertrophy and stabilization Chronic lower back instability Core + pelvic synchronized mode 50–90% 35–45 min 8–12 Lumbopelvic stabilization Table 2.
Technical Characteristics — Alfonse Electromagnetic Platform. Parameter Technical Description Platform Type Multimodal electromagnetic rehabilitation system Electromagnetic Generators 3 independent generators Generator A 3 Tesla pelvic floor stimulation Generator B 2.5 Tesla abdominal/core stimulation Generator C 1.5 Tesla cavernous/perineal stimulation Combined Therapeutic Architecture Simultaneous or independent generator activation Intended Biological Action Supramaximal neuromuscular contraction Target Structures Pelvic floor, core musculature, cavernous/perineal musculature Treatment Method Noninvasive electromagnetic neuromuscular stimulation Energy Delivery Rapid alternating electromagnetic induction Clinical Applications Pelvic rehabilitation, ED support, continence therapy, core strengthening Cooling Requirement Not typically required Patient Interface Chair-based seated therapy system
Figures and Tables
| Clinical Indication | Generator Configuration | Intensity Range | Session Duration | Sessions | Clinical Goal |
|---|---|---|---|---|---|
| Stress urinary incontinence | Pelvic floor generator dominant (3 T) | 40–90% intensity | 28–35 min | 6–10 | Pelvic floor strengthening |
| Pelvic floor rehabilitation | 3 T pelvic generator + 2.5 T core support | 50–95% | 30–40 min | 6–12 | Neuromuscular re-education |
| Erectile dysfunction | 1.5 T cavernous/perineal generator | 40–85% | 25–35 min | 6–10 | Cavernous muscular activation |
| Postpartum pelvic weakness | Combined pelvic + abdominal mode | 35–80% | 30–40 min | 8–12 | Pelvic stability restoration |
| Core strengthening | 2.5 T abdominal generator dominant | 50–100% | 30–45 min | 6–12 | Abdominal hypertrophy and stabilization |
| Chronic lower back instability | Core + pelvic synchronized mode | 50–90% | 35–45 min | 8–12 | Lumbopelvic stabilization |
| Parameter | Technical Description |
|---|---|
| Platform Type | Multimodal electromagnetic rehabilitation system |
| Electromagnetic Generators | 3 independent generators |
| Generator A | 3 Tesla pelvic floor stimulation |
| Generator B | 2.5 Tesla abdominal/core stimulation |
| Generator C | 1.5 Tesla cavernous/perineal stimulation |
| Combined Therapeutic Architecture | Simultaneous or independent generator activation |
| Intended Biological Action | Supramaximal neuromuscular contraction |
| Target Structures | Pelvic floor, core musculature, cavernous/perineal musculature |
| Treatment Method | Noninvasive electromagnetic neuromuscular stimulation |
| Energy Delivery | Rapid alternating electromagnetic induction |
| Clinical Applications | Pelvic rehabilitation, ED support, continence therapy, core strengthening |
| Cooling Requirement | Not typically required |
| Patient Interface | Chair-based seated therapy system |
References
- Jundt K, Peschers U, Kentenich H. The investigation and treatment of female pelvic floor dysfunction. Dtsch Ärztebl Int. 2015;112(33–34):564–574.
- Aoki Y, Brown HW, Brubaker L, et al. Urinary incontinence in women. Nat Rev Dis Primers. 2017;3:17042.
- Lim R, Liong ML, Leong WS, et al. Pulsed magnetic stimulation for stress urinary incontinence: 1-year follow-up results. J Urol. 2017;197(5):1302–1308.
- Yokoyama T, Fujita O, Nishiguchi J, et al. Extracorporeal magnetic innervation treatment for urinary incontinence. Int J Urol. 2004;11(8):602–606.
- Samuels JB, Pezzella A, Berenholz J, et al. Safety and efficacy of non-invasive high-intensity targeted electromagnetic field treatment. Lasers Surg Med. 2019;51(9):760–766.
- Dietz HP. Pelvic floor ultrasound: a review. Am J Obstet Gynecol. 2010;202(4):321–334.
- Bø K, Berghmans B, Mørkved S, et al. Evidence- Based Physical Therapy for the Pelvic Floor. Churchill Livingstone; 2015.
- Glazer HI, Romanzi L, Polaneczky M. Pelvic floor muscle surface electromyography. J Reprod Med. 1999;44(9):779–782.
- Newman DK. Pelvic floor muscle rehabilitation using biofeedback. Urol Nurs. 2014;34(4):193–202.
- Castro RA, Arruda RM, Zanetti MRD, et al. Randomized controlled trial of pelvic floor training and electrical stimulation. Clinics. 2008;63(4):465–472.
- YangS,SangW,FengJ,etal.Pelvicnerveelectrophysiology and tissue function rehabilitation study. J Clin Nurs. 2017;26(23–24):4537–4547.
- Dietz HP, Shek KL. Levator avulsion and pelvic floor ultrasound assessment. Ultrasound Obstet Gynecol. 2008;32(7):941–945.
- Prodanovic M, Malešević J, Filipovic M, et al. Numerical simulation of energy distribution in biological tissues during electrical stimulation. Serbian J Electr Eng. 2013;10:165–173.
- Fowler CJ, Panicker JN, Emmanuel A. Pelvic Organ Dysfunction in Neurological Disease. Cambridge University Press; 2010.
- BøK,TalsethT,HolmeI.Pelvicfloorexerciseandstimulation randomized trial. BMJ. 1999;318(7182):487–493.
This is a text version generated from the article. For the formatted version of record (with original tables & figures), download the PDF →