Full Text Hide / show
Introduction
Postpartum headache is a frequent clinical challenge encountered in obstetric and anaesthetic practice. In the setting of neuraxial anaesthesia, PDPH remains the leading diagnosis and is attributed to inadvertent or intended dural puncture, leading to cerebrospinal fluid (CSF) leakage and intracranial hypotension [1]. However, secondary causes may account for up to 40% of severe postpartum headaches, and these include potentially life-threatening conditions such as eclampsia, PRES, cerebral venous sinus thrombosis (CVST), subarachnoid haemorrhage, and RCVS [2,3]. Reversible Cerebral Vasoconstriction Syndrome (RCVS) is an increasingly recognised condition characterised by multifocal, segmental narrowing of cerebral arteries that typically resolves over days to weeks. Its hallmark clinical feature is recurrent thunderclap headache, but it may also manifest with focal neurological deficits, seizures, stroke, or visual disturbances.
Posterior Reversible Encephalopathy Syndrome (PRES) represents a neuroradiological and clinical syndrome characterised by vasogenic oedema predominantly in posterior cerebral regions, associated with acute hypertension, seizures, encephalopathy, and visual symptoms [4]. Crucially, RCVS and PRES are not mutually exclusive — emerging evidence highlights a spectrum of overlapping pathophysiology involving shared endothelial dysfunction and cerebral autoregulatory failure, especially in the postpartum period [5]. The postpartum state itself is a recognised trigger for both RCVS and PRES, likely mediated by hormonal flux, haemodynamic shifts, sympathetic surges, and circulating vasoactive substances. The added variable of spinal anaesthesia — which alters CSF dynamics, sympathetic tone, and cerebrovascular reactivity — may further predispose susceptible individuals to these phenomena [6].
We report a rare case in which postpartum eclampsia with concurrent RCVS–PRES spectrum disorder initially mimicked PDPH, resulting in a delayed but ultimately successful diagnosis and recovery.
Case Presentation Patient Profile and Initial Presentation A 30-year-old woman (P2L2) with no known antepartum comorbidities was admitted for elective LSCS. She had no prior history of hypertension, pre-eclampsia, renal disease, or neurological illness. The procedure was performed under standard spinal anaesthesia with an uneventful intraoperative course. There were no documented complications at the time of dural puncture and no abnormalities were noted in the immediate post-anaesthetic recovery period. On postoperative day 1, the patient began complaining of persistent headache. At this stage, vital signs remained stable and there were no focal neurological deficits. Given the recent spinal anaesthesia, a provisional diagnosis of PDPH was made, and she was managed conservatively with intravenous hydration, oral analgesics, and close observation.
The headache failed to demonstrate the characteristic postural variation expected in PDPH — notably, it was not relieved by recumbency — and showed no symptomatic improvement over the subsequent 48 hours. Clinical Deterioration On postoperative day 3, a new and unexplained finding emerged: the patient developed significant bradycardia with a pulse rate of 40–44 beats per minute. Blood pressure at this point remained within the normal range, and oxygen saturation was maintained between 92–95% on room air. A 12-lead ECG confirmed sinus bradycardia with no evidence of heart block or ischaemic changes. Two-dimensional echocardiography (2D ECHO) and contrast-enhanced computed tomography (CECT) of the chest and abdomen revealed no structural or pulmonary pathology.
The aetiology of the bradycardia remained unexplained at this stage and, in retrospect, may have represented an early autonomic manifestation of evolving cerebral dysregulation. By postoperative day 5, the clinical picture had escalated substantially. The patient developed acute blurring of vision alongside a sharp rise in blood pressure to 160/100 mmHg. Notably, urine spot protein was negative, and all routine blood investigations — including full blood count, renal and liver function tests, and coagulation profile — remained within normal limits. Given the constellation of persistent headache, visual disturbance, and new-onset hypertension in the postpartum setting, a clinical diagnosis of postpartum eclampsia was entertained. Magnesium sulphate infusion was commenced according to the Zuspan regimen, and intravenous labetalol 20 mg was administered as a stat dose for acute blood pressure control.
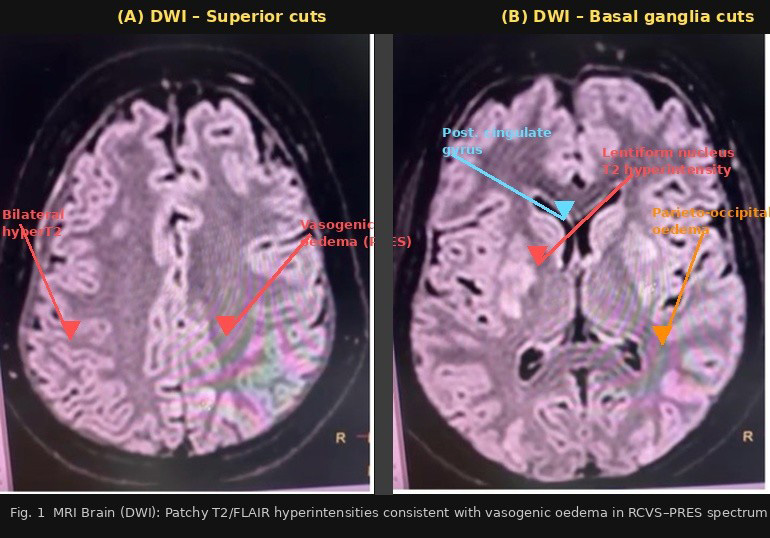
Despitethesemeasures,at11:00hoursthepatientexperienced a single episode of generalized tonic-clonic seizure, following which she was emergently transferred to the Intensive Care Unit (ICU) for close monitoring and further management. Neuroimaging and Final Diagnosis Urgent MRI of the brain was performed and demonstrated patchy areas of T2/FLAIR hyperintensity involving the grey matter of bilateral parieto-occipital regions, the posterior aspect of the cingulate gyrus, bilateral lentiform nuclei, and the body of the right caudate nucleus. These findings were consistent with vasogenic oedema in a distribution characteristic of PRES (Fig 1). The co-occurrence of clinical featuresofcerebralvasoconstriction—inapostpartumpatient withoutpriorhypertension,presentingwithheadache,seizure, and visual disturbance — established the final diagnosis of Postpartum Eclampsia with RCVS–PRES Spectrum Disorder. Figure 1. Treatment and Outcome In the ICU, the patient was continued on magnesium sulphate infusion at 1 g/hour for seizure prophylaxis, supplemental oxygen, and intravenous antibiotics to prevent nosocomial infection.
Intravenous levetiracetam was initiated for seizure control and subsequently transitioned to oral therapy. Nimodipine, a selective calcium channel blocker with established efficacy in cerebral vasospasm, was added to address the vasoconstriction component of RCVS. The patient showed progressive clinical improvement: blood pressure normalised, visual symptoms fully resolved, and no further seizure activity was recorded. She was successfully discharged in a stable neurological condition.
Discussion
Diagnostic Transitions and Clinical Learning Points This case illustrates a challenging sequence of diagnostic transitions that are instructive for both obstetricians and anaesthesiologists. The initial presentation was entirely consistent with PDPH — a well-recognised complication following spinal anaesthesia. However, several atypical features should have prompted earlier re-evaluation. The headache lacked postural character, was unresponsive to conservative therapy, and was later accompanied by neurological symptoms absent in PDPH. The principle that headache following neuraxial anaesthesia is PDPH until proven otherwise is clinically convenient but potentially dangerous, particularly when warning signs evolve. Postpartum eclampsia, which accounts for 20–30% of all eclamptic seizures, is well recognised to occur without antecedent hypertension or proteinuria during the antenatal period, as observed in this patient.
The classical prodrome of persistent headache, followed by visual disturbance, acute hypertension, and finally seizure — though temporally extended over five days in this case — mirrors the established pathophysiological cascade. The absence of proteinuria does not exclude the diagnosis, as endothelial dysfunction and cerebral autoregulatory failure can manifest independently of renal proteinuria [6,7]. The concurrent identification of RCVS–PRES spectrum disorder reflects the growing recognition that these are not isolated entities but rather interrelated expressions of a common pathophysiological substrate. RCVS is characterised by reversible segmental cerebral arterial vasoconstriction with clinical improvement over weeks [8]. PRES reflects the downstream consequence of failed cerebral autoregulation — when arterial pressure overwhelms the vasculature's protective vasoconstriction, breakthrough hyperperfusion and vasogenic oedema ensue.
In the postpartum setting, both are driven by hormonal changes, heightened sympathetic activity, and circulating vasoactive mediators including endothelin-1 and serotonin [9,10]. Role of Spinal Anaesthesia The potential contributory role of spinal anaesthesia in precipitating or unmasking RCVS–PRES in susceptible individuals deserves consideration. Subarachnoid injection alters CSF pressure dynamics acutely, and compensatory cerebrovascular responses to these shifts may trigger vasoreactivity in predisposed vessels [11]. Additionally, the acute sympatholysis following spinal block, and subsequent rebound sympathetic surge during recovery, may contribute to the haemodynamic instability that predisposes cerebral autoregulatory failure. The unexplained bradycardia observed on day 3 may have represented an aberrant autonomic response within this context [12]. Differential Diagnosis and Exclusion The differential diagnosis for this presentation was broad and included PDPH, cerebral venous sinus thrombosis (CVST), intracranial haemorrhage, meningitis, and isolated PRES or RCVS.
CT brain and CT angiography excluded haemorrhagic stroke and significant cerebral venous pathology [13,14]. The characteristic MRI pattern of posterior predominant vasogenic oedema without diffusion restriction, in the context of postpartum onset, acute hypertension, seizure, and clinical recovery with appropriate therapy, cemented the RCVS–PRES diagnosis (Table1) [15]. Table 1. Summary of the key differentiating features between postpartum RCVS and PRES across clinical presentation, neuroimaging, and management — highlighting their overlapping spectrum. Feature Postpartum RCVS Postpartum PRES CLINICAL FEATURES Headache Thunderclap; recurrent, severe Hallmark feature Diffuse, progressive; less abrupt Often gradual onset Seizures Less common (~20–30%) Seen in severe cases Prominent (~60–75%) Often the presenting feature Visual symptoms Transient blurring, scotomata Intermittent Cortical blindness, hemianopia Prominent feature Hypertension Variable; may be absent Not required for diagnosis Typically severe (>160/110 mmHg) Usually present Encephalopathy Uncommon unless stroke complicates Rare Confusion, drowsiness, agitation Common Proteinuria Absent Not a feature Variable; present if eclampsia overlap May be absent Postpartum onset Days to 4 weeks Peak: week 1–2 Usually within 48–72 hours Peak: first 24–72 hrs Course Monophasic; resolves over weeks Generally benign Resolves days–weeks with treatment Reversible IMAGING FINDINGS MRI T2/FLAIR Often normal early May show cortical SAH or infarct later Patchy hyperintensity in parieto-occipital regions Hallmark finding Distribution Anterior > posterior Territorial if infarct present Posterior predominant Parieto-occipital, cerebellar, lentiform nuclei DWI / ADC Restricted diffusion if ischaemic stroke DWI bright / ADC dark Facilitated diffusion (vasogenic oedema) DWI dark / ADC bright MRA / CTA Multifocal segmental vasoconstriction "String-and-beads" pattern Usually normal vessels Vascular imaging unaffected DSA (angiography) Definitive; confirms reversible vasoconstriction Gold standard Typically normal; not required Not a routine investigation Haemorrhage Cortical SAH, lobar ICH possible Significant complication risk Rare haemorrhagic transformation Uncommon MRI enhancement No parenchymal enhancement Typically absent Leptomeningeal enhancement in some cases Occasional finding Imaging reversibility Vasoconstriction resolves in 4–12 weeks Confirm on follow-up MRA Oedema resolves in days–weeks Confirm on followup MRI PATHOPHYSIOLOGY & MANAGEMENT Core mechanism Segmental cerebral arterial vasospasm Vasoconstriction predominates Failed cerebrovascular autoregulation Vasogenic oedema from hyperperfusion CSF findings Normal or mildly elevated protein Near normal Normal Not diagnostic Key treatment Nimodipine (calcium channel blocker) Avoid vasoconstrictors and triptans BP control: labetalol, hydralazine Magnesium sulphate if eclampsia co-exists Prognosis Good; stroke risk if untreated Vigilance for complications Excellent with treatment Rare recurrence
Conclusion
This case powerfully demonstrates that persistent postpartum headache following spinal anaesthesia must not be reflexively attributed to PDPH. A thorough, dynamic clinical re-evaluation is essential whenever headache proves refractory to conservative management, lacks typical postural characteristics, or is accompanied by any neurological symptom — however subtle. The triad of headache, visual disturbance, and hypertension in the postpartum period must raise urgent suspicion for eclampsia and RCVS–PRES spectrum disorder. Timely neuroimaging — particularly MRI with FLAIR sequences — is essential for diagnosis when secondary causes are suspected. Early administration of magnesium sulphate for seizure prophylaxis and prevention of cerebral vasospasm, combined with targeted antihypertensive therapy and calcium channel blockers such as nimodipine to address vasoconstriction, represents the cornerstone of management.
Multidisciplinary collaboration between obstetrics, anaesthesiology, neurology, and critical care is vital in navigating these complex presentations. As RCVS–PRES spectrum disorder becomes increasingly recognised in the postpartum population, awareness among frontline clinicians must keep pace. The maternal outcome in this case was excellent precisely because the diagnosis was ultimately made and treatment escalated appropriately. Vigilance, clinical flexibility, and a willingness to look beyond the most common diagnosis remain the most powerful tools in postpartum neurological care. Acknowledgements Nil Conflict of Interest The authors have no conflicts of interest to disclose.
Figures and Tables
| Feature CLINICAL FEATURES | Postpartum RCVS | Postpartum PRES |
|---|---|---|
| Headache | Thunderclap; recurrent, severe Hallmark feature | Diffuse, progressive; less abrupt Often gradual onset |
| Seizures | Less common (~20–30%) Seen in severe cases | Prominent (~60–75%) Often the presenting feature |
| Visual symptoms | Transient blurring, scotomata Intermittent | Cortical blindness, hemianopia Prominent feature |
| Hypertension | Variable; may be absent Not required for diagnosis | Typically severe (>160/110 mmHg) Usually present |
| Encephalopathy | Uncommon unless stroke complicates Rare | Confusion, drowsiness, agitation Common |
| Proteinuria | Absent Not a feature | Variable; present if eclampsia overlap May be absent |
| Postpartum onset | Days to 4 weeks Peak: week 1–2 | Usually within 48–72 hours Peak: first 24–72 hrs |
| Course IMAGING FINDINGS | Monophasic; resolves over weeks Generally benign | Resolves days–weeks with treatment Reversible |
| MRI T2/FLAIR | Often normal early May show cortical SAH or infarct later | Patchy hyperintensity in parieto-occipital regions Hallmark finding |
| Distribution | Anterior > posterior Territorial if infarct present | Posterior predominant Parieto-occipital, cerebellar, lentiform nuclei |
| DWI / ADC | Restricted diffusion if ischaemic stroke DWI bright / ADC dark | Facilitated diffusion (vasogenic oedema) DWI dark / ADC bright |
| MRA / CTA | Multifocal segmental vasoconstriction "String-and-beads" pattern | Usually normal vessels Vascular imaging unaffected |
| DSA (angiography) | Definitive; confirms reversible vasoconstriction Gold standard | Typically normal; not required Not a routine investigation |
| Haemorrhage | Cortical SAH, lobar ICH possible Significant complication risk | Rare haemorrhagic transformation Uncommon |
| MRI enhancement | No parenchymal enhancement Typically absent | Leptomeningeal enhancement in some cases Occasional finding |
| Imaging reversibility PATHOPHYSIOLOGY & MANAGEMENT | Vasoconstriction resolves in 4–12 weeks Confirm on follow-up MRA | Oedema resolves in days–weeks Confirm on follow- up MRI |
| Core mechanism | Segmental cerebral arterial vasospasm Vasoconstriction predominates | Failed cerebrovascular autoregulation Vasogenic oedema from hyperperfusion |
| CSF findings | Normal or mildly elevated protein Near normal | Normal Not diagnostic |
|---|---|---|
| Key treatment | Nimodipine (calcium channel blocker) Avoid vasoconstrictors and triptans | BP control: labetalol, hydralazine Magnesium sulphate if eclampsia co-exists |
| Prognosis | Good; stroke risk if untreated Vigilance for complications | Excellent with treatment Rare recurrence |
References
- Joudi N, Ansari J. Postpartum headaches after epidural or spinal anesthesia. Curr Opin Obstet Gynecol. 2021 Apr 01;33(2):94-99
- Goldszmidt E, Kern R, Chaput A, Macarthur A. The incidence and etiology of postpartum headaches: a prospective cohort study. Can J Anaesth. 2005 Nov;52(9):971-7.
- Khoromi S. Secondary headaches in pregnancy and the puerperium. Front Neurol. 2023;14:1239078
- Chen SP, Wang SJ. Pathophysiology of reversible cerebral vasoconstriction syndrome. J Biomed Sci. 2022 Sep 21;29(1):72
- Jeanneret V, Jillella DV, Rangaraju S, et al. PRES and RCVS: Two Distinct Entities or a Spectrum of the Same Disease?. J Stroke Cerebrovasc Dis. 2022;31(6):106472. doi:10.1016/j.jstrokecerebrovasdis.2022.106472
- American College of Obstetricians and Gynecologists. Gestational hypertension and preeclampsia. ACOG Practice Bulletin No. 222. Obstet Gynecol. 2020;135(6):e237–e260.
- Stella CL, Jodicke CD, How HY, Harkness UF, Sibai BM. Postpartum headache: is your work-up complete? Am J Obstet Gynecol. 2007;196(4):318.e1–318.e7.
- Sveinsson O, Love Á, Vilmarsson V, Olafsson I. [Reversible cerebral vasoconstriction syndrome - a common cause of thunderclap headache]. Laeknabladid. 2020 Feb;106(2):79-83
- Fugate JE, Rabinstein AA. Posterior reversible encephalopathy syndrome: clinical and radiological manifestations, pathophysiology, and outstanding questions. Lancet Neurol. 2015;14(9):914–925.
- Bartynski WS. Posterior reversible encephalopathy syndrome, Part 2: controversies surrounding pathophysiology of vasogenic edema. AJNR Am J Neuroradiol. 2008;29(6):1043–1049
- Safran SL, Balmer C, Savoldelli G. Reversible cerebral vasoconstriction syndrome during caesarean section. BMJ Case Rep. 2019 Dec 5;12(12):e230606. doi: 10.1136/ bcr-2019-230606.
- Doelakeh ES, Chandak A. Risk Factors in Administering Spinal Anesthesia: A Comprehensive Review. Cureus. 2023 Dec 4;15(12):e49886. doi: 10.7759/cureus.49886
- Perillo T, Paolella C, Perrotta G, Serino A, Caranci F, Manto A. Reversible cerebral vasoconstriction syndrome: review of neuroimaging findings. Radiol Med. 2022 Sep;127(9):981-990
- Ducros A, Boukobza M, Porcher R, Sarov M, Valade D, Bousser MG. The clinical and radiological spectrum of reversible cerebral vasoconstriction syndrome. A prospective series of 67 patients. Brain. 2007 Dec;130(Pt 12):3091-101
- Bartynski WS. Posterior reversible encephalopathy syndrome, Part 1: fundamental imaging and clinical features. AJNR Am J Neuroradiol. 2008;29(6):1036–1042
This is a text version generated from the article. For the formatted version of record (with original tables & figures), download the PDF →