Full Text Hide / show
Background
: Juvenile idiopathic arthritis (JIA) is treated with methotrexate (MTX), but its adverse effects can lead to treatment discontinuation. This study investigates the incidence and risk factors of MTX side effects in JIA patients. Methods: A retrospective study of 123 JIA patients (aged 1-18 years) treated with MTX between 2002 and 2020 was conducted. Results: 78.9% of patients experienced MTX side effects. Younger patients (<5 years) had higher rates of upper respiratory tract infections. Tablet-administered MTX was associated with increased vomiting, mouth ulcers, low platelet counts, and anemia. Concomitant treatments with MTX were linked to higher vomiting and abdominal pain. Longer treatment duration correlated with elevated liver enzymes and vomiting.
Patients and Methods
with poor compliance had a significantly higher incidence of side effects (67%) compared to those with good compliance (33%). Conclusions: MTX treatment for JIA is associated with significant side effects, varying by patient factors and treatment methods. Understanding these risks is critical for optimizing treatment and minimizing negative outcomes. Further research is needed to explore strategies for mitigating adverse effects and improving patient compliance. Keywords: Juvenile Idiopathic arthritis, Methotrexate, adverse effects, Pediatric Rheumatology.
Introduction
Juvenile Idiopathic Arthritis (JIA) is the most common chronic rheumatic disease in children and teens, characterized by joint pain and inflammation. The international standard, established by the International League of Associations for Rheumatology (ILAR), categorizes JIA into seven mutually exclusive subtypes, including oligoarticular, polyarticular, systemic JIA, psoriatic JIA, and enthesitis-related JIA [1, 2]. Symptoms vary widely but may include high fever, rash, and enlarged lymph nodes, particularly in the systemic subtype [3]. JIA can also affect the eye, causing uveitis, the most common cause of blindness in these patients. Methotrexate (MTX) is the cornerstone of JIA management and is the recommended first-line conventional Disease-Modifying Anti-Rheumatic Drug (DMARD), managing arthritis symptoms and preventing long-term joint damage [4-6].
Symptom improvement usually occurs within 6–12 weeks [7]. MTX's therapeutic efficacy stems from multiple complex mechanisms, positioning it as the global standard for rheumatoid diseases due to its efficacy and low cost [8, 9]. MTX inhibits dihydrofolate reductase (DHFR), an enzyme essential for converting dihydrofolate to tetrahydrofolate (THF). This suppresses the immune response by reducing the production of purines and pyrimidines, which are vital for DNA and RNA synthesis in rapidly proliferating immune cells involved in JIA [9, 10]. MTX also increases extracellular adenosine levels, which exerts powerful anti-inflammatory effects [9]. Its efficacy is also attributed to the regulation of inflammatory signaling, promotion of bone protection, and maintenance of overall immune system function [9].
Despite its efficacy, MTX is associated with a wide range of side effects that pose a significant barrier to successful treatment. The necessity of using a folate antagonist requires co-administration of folic acid supplementation to mitigate common side effects like nausea and stomatitis (mouth ulcers) [11]. MTX can cause various adverse effects, including; Common Gastrointestinal Symptoms such as nausea (occurring in about 10% of patients), stomatitis (up to one-third of patients), abdominal pain, and vomiting. Serious toxicities as liver problems (hepatotoxicity), lung problems (pulmonary toxicity), and hematologic toxicity (low blood cell counts, including leukopenia, thrombocytopenia, and megaloblastic anemia) [11]. MTX's role has evolved due to the introduction of biologic DMARDs, but it remains the preferred initial therapy [11, 12].
The management challenge now lies in minimizing adverse effects to ensure patient adherence. Furthermore, the pharmacokinetics of MTX exhibit significant intersubject variability [15-17]. This variability is influenced by multiple factors, including dose-dependent absorption, body surface area, renal function, volume of distribution, route of administration, and genetic mutations [13-17]. While studies on adults with rheumatoid arthritis have identified that age, body weight, creatinine clearance, gender, dose, and fasting status significantly affect MTX absorption [13, 14], data in the pediatric population show specific differences—for instance, pediatrics experience a decline in absorption at doses above 40 mg/m2, whereas adults experience it above 80 mg/m2 [18]. Additionally, children may face difficulties in treatment compliance and require specific tools to predict methotrexate intolerance [19-20].
Given the frequency and significance of adverse effects, and the need for optimal, long-term adherence in JIA patients. Thus, this study aims to analyze the adverse effects of methotrexate (MTX) in patients with juvenile idiopathic arthritis, identify factors influencing their development, evaluate the treatment's longterm safety, and assess its impact on patient compliance.
Methodology
The study involving 123 patients aged 1-18 years with juvenile arthritis (JIA) from 2002 to 2020 at Al-Jala Pediatric Hospital examined the adverse effects of MTX treatment. The study assessed gastrointestinal, hepatic, hematologic, infectious, and mouth ulcer effects. Liver function tests and blood account tests were also recorded at least one month after treatment initiation and every three to four months thereafter. Patients used other medications combined with MTX to control the disease. Statistical analysis The study used descriptive statistics, chi-square test, student's t-test, and Kaplan-Meier survival analysis to analyze the effects of methotrexate on patients. The results were presented in tables and graphs, and statistical significance was defined as a p-value of less than or equal to 0.05. The study assessed the association between categorical variables and the duration of mean survival.
Results
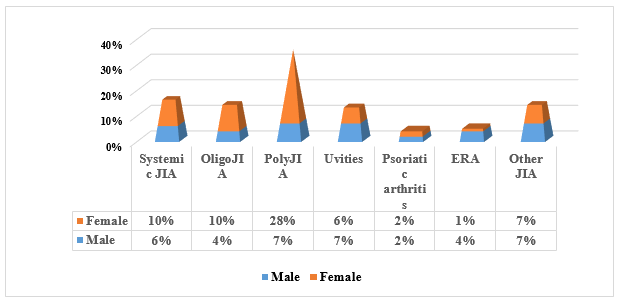
The sample's basic epidemiological characteristic is as follows: The study included 123 patients: 78 female (63.4%) and 45 male (36.6%) as illustrated in (Table 1). The mean age at treatment start was 7.6 years (S.D ± 4) (Table 1). Patients were classified based on the ILAR criteria (Fig. 1), This found that 43 patients have poly arthritis (35%), systemic arthritis 19 patients (15.4%), oligo arthritis 17 patients (13.8%), 5 patients with psoriatic arthritis (4.1%), patient with ERA 6 (4.9%), 16 patients with uveitis (13%), and 17 patients are diagnosed with other diseases (13.8%).The mean of the doses of methotrexate used was 13.6 mg/m2/week (S.D ±2.4) (Table 1). In addition, 93 of patients administered MTX subcutaneously (represent 76%) while only 30 patients taken the drug orally (24%) (Table 1).
The mean of duration of treatment was 3.9 years (S.D ±2.2) (Table 1), whereas other treatment used with MTX was recorded in 72 patients (58.6%). In the meantime, 25 of patients (20%) were treated with prednisolone, whereas 12 of patients were treated with naproxen (10%), 7 patients (6%) were treated with naproxen and prednisolone, 28 patients treatedwithbiologyand51patientsonMTXalone(41%)(Fig.1). Figure 1. Different types of juvenile idiopathic arthritis according to gender. The frequency and type of adverse drug reactions Ninety-seven (n= 97, 78.9%) patients experienced side effects during MTX treatment, with 35% experiencing vomiting and 34% experiencing high liver enzyme. The least common type was pneumonia infection (4%), with a mean duration of 1.3 years for adverse reactions (Table 2).
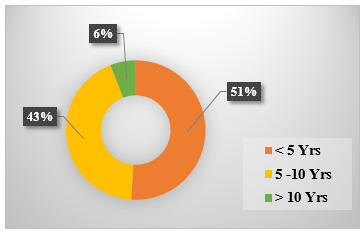
Table 1. Displays the age, sex, doses, duration, and administration routes of MTX treatment in relation to the number of patients with JIA. Item N Percent Mean SD Age group >5 years 6-12 years 13-18 years 37 % 49 % 14% 7.6 Sex Male Female 36.6% 63.4% Doses 10 (mg/m2) 11-15 (mg/m2) 16 (mg/m2) 25% 70% 5% 13.6 mg/m2 S.D ±2.4 MTX treatment duration Less than 1 year 1- 3 years Above 3 years 10 % 39 % 51% 3.9 year S.D ±2.2 Route of administration Tablet Subcutanious 24% 76% Table 2. Includes general information on the number of JIA patients who experienced side effects, those who continued treatment, and those who discontinued treatment.
Parameters Percent Patients having adverse effects Yes No 79% 21% Patients on MTX Stay on Treatment Discontinue it 59% 41% No. of Side effects One side effect Two or more ≥ Two side effect Upper respiratory tract infection < 5 Yrs 24% 5 -10 Yrs 20 > 10 Yrs 2% The highest side effect Vomiting High liver enzyme Pneumonia 35% 34% 4% Factors associated with adverse reactions are This study identified several demographic and treatment-related variables that significantly influenced the incidence and type of adverse reactions experienced by Juvenile Idiopathic Arthritis (JIA) patients treated with Methotrexate (MTX). The factors investigated included age, gender, dose, route, treatment duration, and concomitant medications (as summarized in Table 1).
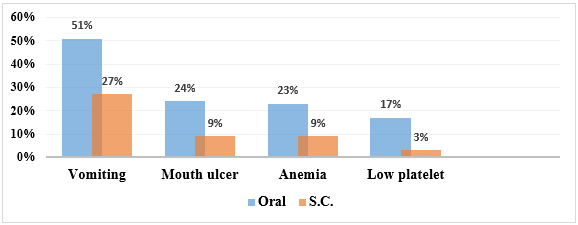
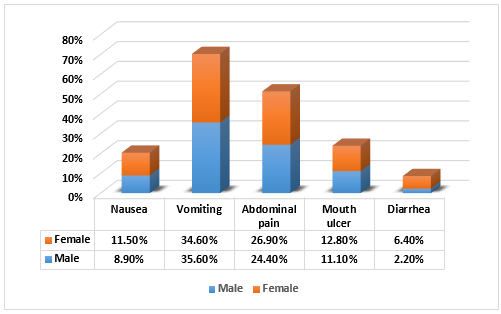
Demographic Factors (Age and Gender) • Age at Treatment Initiation: A significant association was found between the patient's age at MTX initiation and the occurrence of upper respiratory tract infections (URTIs). Patients under 5 years old experienced URTIs more than twice per year during MTX treatment compared to older patients. • Gender: No statistically significant association was observed between gender and the overall incidence of adverse effects. Treatment-Related Factors Route of Administration Table 3 and 4 summarize the association between concomitant treatments/treatment duration and specific adverse effects of Methotrexate (MTX). Table 3. The route of MTX administration showed a clear association with Gastrointestinal (GIT) side effects and hematological adverse reactions: Side Effect Oral (Tablet) Route Subcutaneous (Injection) Route Findings Vomiting 51.2% 26.8% Oral administration resulted in significantly higher rates of vomiting.
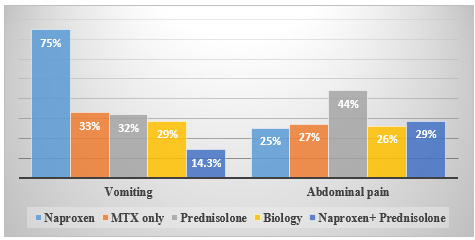
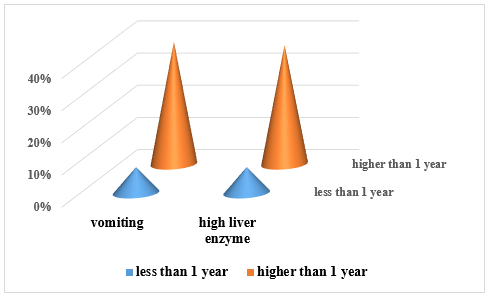
Mouth Ulcers (Stomatitis) 24.0% 8.5% Oral administration resulted in significantly higher rates of mouth ulcers. Table4.summarizesthepercentageofpatientsexperiencingvomitingwhenMTXwasadministeredaloneversusincombination with other common treatments for Juvenile Idiopathic Arthritis (JIA). Concomitant Treatment Group Vomiting Incidence Patients taking other treatments (Overall) 75 % Prednisolone only 32 % Naproxen and Prednisolone 14.3 % Biologics 28.6 % No other treatment (MTX monotherapy) 33.3 % The study found a significant association indicating that the risk of elevated liver enzymes increases substantially with MTX treatment lasting more than one year (36.9% vs. 8.3%) (Table 5). Table 5. Summarizes the significant association found between the duration of MTX treatment and the incidence of high liver enzymes. Duration of MTX Treatment High Liver Enzymes Incidence (Hepatotoxicity) Vomiting Incidence Less than 1 year 8.3% 8.3% More than 1 year 36.9% Not specified in data Discontinuation of treatment and patient’s compliance The outcomes for the 40.7% of patients who discontinued MTX after a mean follow-up duration of 3.9 years were summarized in table 6.
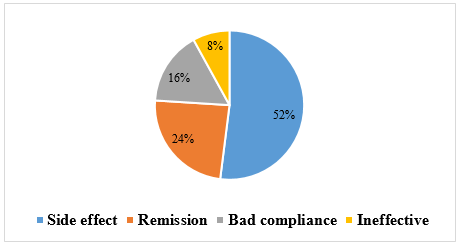
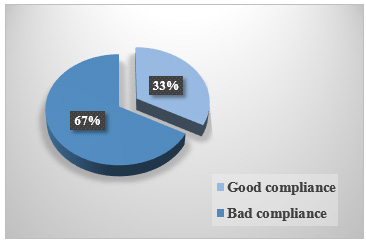
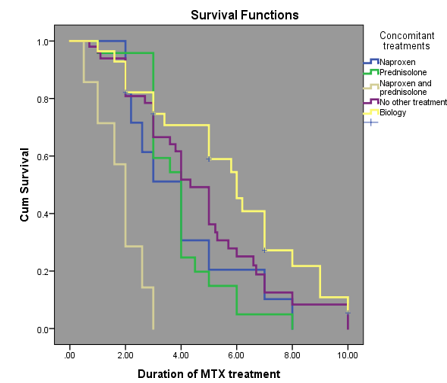
Data is based on 26 patients whose reasons for stopping were analysed. Reasons for discontinuation included adverse effects (52%), remission (24%), bad compliance (16%), and ineffectiveness (8%) in 26 patients. The most common adverse effect was GIT adverse effect in these 26 patients. The Kaplan Meier method was used to compare the treatment duration until discontinuation due to side effects between methotrexate alone and other treatments. the MTX and biology treatment showed the highest survival rate, with the probability of continuing treatment up to 8 years (20%), 8% (MTX alone), 10% MTX with naproxen, 15% (MTX and prednisolone), and 15% MTX with naproxen and prednisolone. In table 7, Patients with poor compliance experienced higher adverse effects (67%) during treatment compared to those with good compliance (33%).
Table 6. Reasons for MTX Treatment Discontinuation. Reason for Discontinuation Percentage of Discontinued Patients (n=26) Adverse Effects 52 % Remission 24 % Bad Compliance 16 % Ineffectiveness 8 % Table 7. Treatment Continuation Probability and Compliance Effects This table summarizes the treatment survival (continuation) probability at 8 years based on treatment regimen, and the relationship between patient compliance and adverse effects. Factor Detail Probability/Incidence Probability of Continuing MTX (Survival Rate) at 8 Years MTX with Biologic therapy 20% (Highest) MTX with Prednisolone 15% MTX with Naproxen and Prednisolone 15% MTX with Naproxen 10% MTX alone 8% (Lowest) Adverse Effects based on Patient Compliance Patients with Poor Compliance 67% incidence of adverse effects Patients with Good Compliance 33% incidence of adverse effects Figure 2.
Compares the severity of MTX side effects depending on route of administration. Figure 3. Comparison of the side effects of MTX with concurrent medication drugs. Figure 4. Depicts the MTX remission rate, side effects, poor compliance, and ineffectiveness, as shown in the accompanying figure. Figure 5. The effect of gender on adverse drug reaction. Figure 6. The strength of side effects by duration of treatment. Figure 7. Shows patient compliance. Figure 8. Shows patient compliance. Figure 9. Time elapsed from initiation of MTX treatment to discontinuation. Analyzed with the Kaplan Meier method different line colors represent MTX alone and MTX with concomitant treatment. The different coloured lines represent the MTX regimen the patient was receiving.
The higher a curve is, the better the "survival" (i.e., the longer the patient continued treatment). The Kaplan-Meier Survival Curve showing the probability of patients continuing Methotrexate (MTX) treatment over time, which means it tracks the duration of treatment until discontinuation. At 4 years, 68% of patients on biological treatment, 50% on MTX alone, and 25% on Prednisolone are still receiving treatment. By 8 years, the figures drop to approximately 20% for biological treatment and 8% for MTX alone, correlating with survival rates of 20% and 8% respectively (Fig. 9). The graph visually reinforces the finding that the addition of biologic agents is the strongest factor in maintaining patients on MTX treatment over the long term, while the combination with prednisolone has the highest discontinuation risk.
Table 8. The differences in dosage mean between patients with side effects and those without. Adverse effects N Mean S. D t P value Vomiting Yes No 13.8 13.3 2.27390 2.59346 1.096 0.276 Nausea Yes No 13.4 13.7 3.29181 2.47760 -0.272 0.786 Abdominal pain Yes No 13.5 13.6 2.41494 2.56248 -0.278 0.782 Mouth ulcer Yes No 13.4 13.6 1.98969 2.54055 -0.303 0.763 Diarrhea Yes No 14.3 13.6 1.11430 2.50285 1.403 0.825 URTI Yes No 13.2 13.6 3.54467 2.49102 -0.629 0.531 Pneumonia Yes No 14.4 13.7 6.94082 2.43978 0.236 0.825 Herpes zoster Yes No 12.7 13.7 2.29819 2.46273 -0.915 0.362 Chicken pox Yes No 12.1 13.7 4.13382 2.36882 -1.216 0.253 High Liver Enzyme Yes No 14.3 13.3 2.95909 2.56938 1.913 0.058 Low WBC Yes No 14.1 13.6 1.86006 2.49519 .546 0.586 Low platelet Yes No 14.0 13.6 1.86006 2.49519 0.546 0.586 This table presents the results of t-tests comparing the mean Methotrexate (MTX) dosage between two groups for various adverse effects: patients who experienced the side effect (Yes) and those who did not (No).
MTX dosage was not a statistically significant factor in the incidence of any of the tested adverse effects, with one notable exception that approached significance. The statistical analysis performed using the t-test indicated that the mean MTX dose (measured in mg/m2/week, though units are not specified) did not significantly differ between patients who experienced adverse effects and those who did not for nearly all categories tested. For common side effects such as vomiting, nausea, abdominal pain, mouth ulcers, diarrhoea, upper respiratory tract infections (URTI), and various haematological effects (low WBC, low platelets), the P value was consistently above the standard significance level of 0.05 (ranging from 0.253 to 0.825). This suggests that varying the dose within the range used in this study did not increase the likelihood of developing these side effects.
The only adverse effect that showed a near-significant difference was High Liver Enzymes, with a P value of 0.058. While this technically remains above the 0.05 threshold, it is very close and suggests a trend toward a higher mean dose in the group experiencing liver enzyme elevation (14.3) compared to the group without (13.3). This near-significance highlights that dose may be a factor in hepatotoxicity, though further study is warranted to confirm this relationship. In summary, the study demonstrates that the incidence of most MTX adverse effects is largely independent of the mean weekly dose administered.
Discussion
The study investigates the use of methotrexate (MTX) in treating rheumatoid arthritis (JIA) in pediatric and adolescent patients. As known MTX's mechanisms include adenosine signaling modulation, cytokine network alteration, reactive oxygen species generation, and suppression of High-mobility group box protein 1 (HMGB1)- alarmin. Despite potential to attenuate immune surveillance, MTX remains a key treatment. Risk factors for treatment toxicity and adverse effects and longer therapy duration remains a crucial issue. This study reveals that female patients with juvenile idiopathic arthritis (JIA) have a higher percentage of adverse effects than male patients, which is consistent with previous studies. The age at presentation for JIA is similar to other studies, with a median age of 6.4 years.
The most common types of JIA are polyarthritis and oligo arthritis. The study examines the frequency and types of adverse effects associated with methotrexate (MTX) treatment in Libyan patients and describes treatment survival and adverse effect occurrence in children receiving MTX for JIA. There is a lack of published evidence on the importance of methotrexate dose and route of administration on both its efficacy and adverse events in children with JIA. The overall incidence of adverse effects is high, with more than half of the patients reporting one or more side effects from MTX. The most frequent side effects observed in this study were elevated liver enzymes (34%), vomiting (35%), and abdominal pain (26%).
This is consistent with other research reporting occurrences between 21% and 73%. The incidence of GI discomfort and elevated liver enzymes is high, with a high level of GI disturbance caused by MTX. Haematological abnormalities described in this study include significantly decreased blood counts: anemia (12%), low WBC (6.5%), and low platelets (6.5%). Methotrexate hematological complications are known, but every study agrees on reporting a low frequency of these events. MTX is associated with the development of opportunistic infections, with the incidence of pneumonia infection being the lowest at 4%. However, the overall infection rate in this study is considered higher compared to others [21-22]. MTX can also be effective in treating chronic JIA-associated uveitis [23].
MTX and biologic agents are commonly prescribed for JIA treatment, with MTX being a conventional DMARD that suppresses immune response by inhibiting nucleotide synthesis [11]. Biologic agents, such as TNF inhibitors and non- TNF biologics, are reserved for specific cases and can reduce disease activity and improve remission when combined with MTX [24]. However, they have similar adverse event rates compared to MTX alone [11,24]. Vaccinations in JIA patients should be considered based on individual risk and benefit assessments [25]. The study provides valuable insights into the adverse effects of MTX treatment in JIA, suggesting future research should explore long-term safety and effectiveness of interventions to mitigate side effects. The findings could inform treatment decisions and patient education.
Conclusion
Side effects of methotrexate (MTX) are a major concern for patients, leading to discontinuation of many treatments. Contributing factors include dosing errors, metabolic syndrome, hypoalbuminemia, respiratory tract infection, lack of folic acid supplementation, and concomitant use of interacting medications. Combining MTX with TNF or non-TNF biologics reduces disease activity and improves remission compared with MTX monotherapy. Overall adverse events and discontinuation rates were similar between treatment groups. The most common adverse effect leading to discontinuation was Gastrointestinal (GIT) adverse effects. The study focused primarily on adverse effects, but including measures of treatment effectiveness and patient quality of life would provide a more comprehensive understanding of the impact of MTX.
Limitation limitations of the study, such as its retrospective design, the potential for recall bias, or the relatively small sample size. It also lacks a control group, may not fully capture the complex interactions between MTX and other drugs. Study limitations may affect the ability to determine causality and control for confounding variables. Conflict of interest statement The authors declare no conflict of interest.
Figures and Tables
| Item | N | Percent | Mean | SD |
|---|---|---|---|---|
| Age group >5 years 6-12 years 13-18 years | 37 % 49 % 14% | 7.6 | ||
| Sex Male Female | 45 78 | 36.6% 63.4% | ||
| Doses 10 (mg/m2) 11-15 (mg/m2) 16 (mg/m2) | 25% 70% 5% | 13.6 mg/m2 | S.D ±2.4 | |
| MTX treatment duration Less than 1 year 1- 3 years Above 3 years | 10 % 39 % 51% | 3.9 year | S.D ±2.2 | |
| Route of administration Tablet Subcutanious | 30 93 | 24% 76% |
| Parameters | Percent |
|---|---|
| Patients having adverse effects Yes No | 79% 21% |
| Patients on MTX Stay on Treatment Discontinue it No. of Side effects One side effect Two or more ≥ Two side effect Upper respiratory tract infection < 5 Yrs 24% 5 -10 Yrs 20 > 10 Yrs 2% | 59% 41% |
| The highest side effect Vomiting High liver enzyme Pneumonia | 35% 34% 4% |
| Side Effect | Oral (Tablet) Route | Subcutaneous (Injection) Route | Findings |
|---|---|---|---|
| Vomiting | 51.2% | 26.8% | Oral administration resulted in significantly higher rates of vomiting. |
| Mouth Ulcers (Stomatitis) | 24.0% | 8.5% | Oral administration resulted in significantly higher rates of mouth ulcers. |
| Concomitant Treatment Group | Vomiting Incidence |
|---|---|
| Patients taking other treatments (Overall) | 75 % |
| Prednisolone only | 32 % |
| Naproxen and Prednisolone | 14.3 % |
| Biologics | 28.6 % |
| No other treatment (MTX monotherapy) | 33.3 % |
| Duration of MTX Treatment | High Liver Enzymes Incidence (Hepatotoxicity) | Vomiting Incidence |
|---|---|---|
| Less than 1 year | 8.3% | 8.3% |
| More than 1 year | 36.9% | Not specified in data |
| Reason for Discontinuation | Percentage of Discontinued Patients (n=26) |
|---|---|
| Adverse Effects | 52 % |
| Remission | 24 % |
| Bad Compliance | 16 % |
| Ineffectiveness | 8 % |
| Factor | Detail | Probability/Incidence |
|---|---|---|
| Probability of Continuing MTX (Survival Rate) at 8 Years | MTX with Biologic therapy | 20% (Highest) |
| MTX with Prednisolone | 15% | |
| MTX with Naproxen and Prednisolone | 15% | |
| MTX with Naproxen | 10% | |
| MTX alone | 8% (Lowest) | |
| Adverse Effects based on Patient Compliance | Patients with Poor Compliance | 67% incidence of adverse effects |
| Patients with Good Compliance | 33% incidence of adverse effects |
| Adverse effects | N | Mean | S. D | t | P value | |
|---|---|---|---|---|---|---|
| Vomiting | Yes No | 43 80 | 13.8 13.3 | 2.27390 2.59346 | 1.096 | 0.276 |
| Nausea | Yes No | 13 110 | 13.4 13.7 | 3.29181 2.47760 | -0.272 | 0.786 |
| Abdominal pain | Yes No | 32 91 | 13.5 13.6 | 2.41494 2.56248 | -0.278 | 0.782 |
| Mouth ulcer | Yes No | 15 108 | 13.4 13.6 | 1.98969 2.54055 | -0.303 | 0.763 |
| Diarrhea | Yes No | 6 117 | 14.3 13.6 | 1.11430 2.50285 | 1.403 | 0.825 |
| URTI | Yes No | 20 103 | 13.2 13.6 | 3.54467 2.49102 | -0.629 | 0.531 |
| Pneumonia | Yes No | 5 118 | 14.4 13.7 | 6.94082 2.43978 | 0.236 | 0.825 |
| Herpes zoster | Yes No | 6 117 | 12.7 13.7 | 2.29819 2.46273 | -0.915 | 0.362 |
| Chicken pox | Yes No | 10 113 | 12.1 13.7 | 4.13382 2.36882 | -1.216 | 0.253 |
| High Liver Enzyme | Yes No | 42 81 | 14.3 13.3 | 2.95909 2.56938 | 1.913 | 0.058 |
| Low WBC | Yes No | 8 115 | 14.1 13.6 | 1.86006 2.49519 | .546 | 0.586 |
| Low platelet | Yes No | 8 115 | 14.0 13.6 | 1.86006 2.49519 | 0.546 | 0.586 |
References
- Petty RE, Southwood TR, Manners P, et al. International League of Associations for Rheumatology classification of juvenile idiopathic arthritis: second revision, Edmonton, 2001. J Rheumatol. 2004;31(2):390-392.
- Ravelli A, Martini A. Juvenile idiopathic arthritis. Lancet. 2007;369(9563):767-778.
- Thon V, Cinek O. Oligoarticular and polyarticular JIA: epidemiology and pathogenesis. Autoimmun Rev. 2013;12(11):1083-1088.
- Giannini EH, Brewer EJ, Kuzmina N, et al. Methotrexate in resistant juvenile rheumatoid arthritis: results of the U.S.A.-U.S.S.R. double-blind, placebo-controlled trial. N Engl J Med. 1992;326(16):1043-1049.
- FavalliEG,BiggioggeroM,MeroniPL.Methotrexateforthe treatment of rheumatoid arthritis in the biologic era: still an "anchor" drug?. Autoimmun Rev. 2014;13(11):1102- 1108. doi: 10.1016/j.autrev.2014.08.026
- Bedoui Y, Guillot X, Sélambarom J, et al. Methotrexate an Old Drug with New Tricks. Int J Mol Sci. 2019;20(20):5023. Published 2019 Oct 10. doi:10.3390/ijms20205023
- Godfrey C, Sweeney K, Miller K, Hamilton R, Kremer J. The population pharmacokinetics of long-term methotrexateinrheumatoidarthritis.BrJClinPharmacol. 1998;46(4):369-376. doi:10.1046/j.1365-2125.1998 t 01- 1- 00790.x.
- Zhao Z, Hua Z, Luo X, et al. Application and pharmacological mechanism of methotrexate in rheumatoid arthritis. Biomed Pharmacother. 2022; 150:113074. doi: 10.1016/j.biopha.2022.113074
- Cronstein BN, Aune TM. Methotrexate and its mechanisms of action in inflammatory arthritis. Nat Rev Rheumatol. 2020;16 (9):515-527.
- WeinsteinA,ManziS,Methotrexate:MechanismofAction and Clinical Use. Ann Intern Med. 1990;113(12):988-995.
- Ruperto N, Lovell DJ, Methotrexate in Juvenile Idiopathic Arthritis: Advice and Recommendations from the MARAJIA Expert Consensus Meeting. Rheumatol Ther. 2018;5(2):161-178.
- Guzman J, Oen K, Tucker LB, et al. The outcomes of juvenile idiopathic arthritis in children managed with contemporary treatments: results from the ReACCh- Out cohort. Ann Rheum Dis. 2015;74(10):1854-1860.
- Jansen G, The Antirheumatic Action of Methotrexate: The Role of Pharmacogenetics, Membrane Transport, and Metabolism. Semin Arthritis Rheum. 2004;33(5): S39-S45.
- RodenburgK,KilsdonkE,vandenBoschOFC,etal.Factors influencing the oral bioavailability of methotrexate in patients with rheumatoid arthritis: a systematic review. Rheumatology (Oxford). 2018;57(5):824-835.
- Raja A, Anic K. Methotrexate and its therapeutic efficacy in rheumatoid arthritis: the role of genetic variants. Pharmgenomics Pers Med. 2018; 11:21-30.
- Klamp W, Wagner T, Methotrexate pharmacokinetics and route of administration in rheumatology. Clin Exp Rheumatol. 2004;22(2):S45-S49.
- Ferrara G, Mastrangelo G, Barone P, et al. Methotrexate in juvenile idiopathic arthritis: advice and recommendations from the MARAJIA expert consensus meeting. Pediatr Rheumatol Online J. 2018;16(1):46. Published 2018 Jul 11. doi:10.1186/s12969-018-0255-8
- Yang Y, Liu Z, Chen J, Wang X, Jiao Z, Wang Z. Factors influencing methotrexate pharmacokinetics highlight the need for individualized dose adjustment: a systematic review. Eur J Clin Pharmacol. 2024;80(1):11- 37. doi:10.1007/s00228-023-03579-0
- Livermore P. Juvenile idiopathic arthritis: updated guide toadministeringmethotrexate.NursChildYoungPeople. 2014;26(1):26-29. doi:10.7748/ncyp2014.02.26.1.26 e393.
- Donahue, K.E., Schulman, E.R., Gartlehner, G. et al. Comparative Effectiveness of Combining MTX with Biologic Drug Therapy Versus Either MTX or Biologics Alone for Early Rheumatoid Arthritis in Adults: a and Network Meta-analysis. J Gen Intern Med 34, 2232–2245 (2019). https://doi org/10.1007/s11606-019-05230-0
- Smilutė G, Stropuviene K, Infectious complications in juvenile idiopathic arthritis patients treated with methotrexate. Medicina (Kaunas). 2012;48(1):15-20.
- Ringsberg V, Berntson L, Infections in juvenile idiopathic arthritis patients on methotrexate: a follow-up study of the Swedish patient cohort. Pediatr Rheumatol Online J. 2015; 13:17.
- Rabinovich CE, Methotrexate and JIA-associated uveitis: An update on efficacy and safety. Pediatr Rheumatol Online J. 2011;9(1):15.
- Lovell DJ, Giannini EH, Reiff A, et al. Long-term efficacy and safety of etanercept in children with polyarticularcourse juvenile rheumatoid arthritis: results after 10 years. Arthritis Rheum. 2013;65(9):2494-2503.
- Pringsheim T, Vaccination of children with juvenile idiopathic arthritis: a systematic review and metaanalysis of the evidence. Pediatrics. 22005;116(3): e600-e617.
This is a text version generated from the article. For the formatted version of record (with original tables & figures), download the PDF →