Full Text Hide / show
Background
: The intraperitoneal administration of local anesthetics has emerged as a promising adjunct technique to improve postoperative analgesia in abdominal surgeries, including cesarean sections. Objective: to evaluate the efficacy and safety of intraperitoneal local anesthetic administration in reducing postoperative pain and side effects in women undergoing cesarean section Methods: We performed a systematic review and meta-analysis including randomized clinical trials between January 1st 1985 and January 15th 2026 in the PubMed, Embase and Cochrane CENTRAL databases. Results:Atotal of 1220 women were allocated to this meta-analysis. The VAS at 4 hours had a reduction of 15.28 points in favors to intraperitoneal local anesthetic (IPLA) group (I2=0%). VAS at 6, 12 and 24 hours did not demonstrate differences between the groups and showed a high heterogeneity.
Postoperative nausea and vomiting (PONV) showed a reduction of 45% in favors to intervention group (I2=0%). Side effects showed almost half reduction to IPLA group (I2=19%). Opioid need at 24 hours had a 47% reduction to IPLA group with moderate heterogeneity (I2=49%). Satisfaction (I2=93%) and time to first opioid rescue (I2=100%) showed high heterogeneity and no differences between the groups. Discussion: IPLA is a simple and low-cost adjunct that appears most useful for improving early postoperative recovery-reducing pain at 4 hours and decreasing PONV, side effects and opioid rescue needs. However, durability of analgesic benefit beyond the early postoperative window remains uncertain and likely contingent upon co-interventions and technique. Keywords: Cesarean Section; Injections, Intraperitoneal; Postoperative Pain; Anesthetics, local; Meta-Analysis; Postoperative Nausea and Vomiting; Adverse Effects;
Introduction
The frequency of cesarean delivery has increased in recent years, exceeding the 10%–15% rate of historically recommended by the World Health Organization. In a 2021 analysis 1 , the five countries with the highest cesarean rates were the Dominican Republic (58.1%), Brazil (55.7%), Cyprus (55.3%), Egypt (51.8%), and Turkey (50.8%), while the global rate was 21.1%. Projections suggest that the global rate may approach 30% 1 in 2030, underscoring the need to optimize perioperative care for this procedure. Chronic pain after cesarean delivery can persist for at least 3 months, and may last 6–12 months in a subset of women . Acute postoperative pain is common and is associated with adverse outcomes such as delayed mobilization, venous thromboembolism and wound complications 3 .
Postcesarean pain is also influenced by psychosocial factors (e.g., age, educational level, parity, history of infertility, and cultural context), which can affect daily activities and newborn care 4 . The current standard for cesarean anesthesia is regional anesthesia, particularly spinal anesthesia, which commonly includes intrathecal local anesthetic and opioid (e.g., bupivacaine and morphine) 5 . Although this approach provides effective intraoperative anesthesia, many women experience moderate-to-severe postoperative pain, especially within the first 24–48 hours 6 . Despite multimodal analgesia – including nonsteroidal anti-inflammatory drugs and systemic opioids – a substantial proportion of patients still report inadequate pain control, highlighting the need for adjunct strategies 7 . Intraperitoneal instillation of local anesthetic has been explored as an adjunct technique to improve postoperative analgesia in intra-abdominal surgery, including cesarean sections 8,9 .
By irrigating the peritoneal cavity with local anesthetic agents at the end of surgery, it is hypothesized that nociceptive transmission from the visceral and parietal peritoneum may be attenuated, potentially reducing early postoperative pain 9 . However, heterogeneity in protocols (agent, dose, volume, timing, and concomitant analgesia) and differences in pain assessment limit generalizability across studies. A focused systematic review and meta-analysis of randomized trials is needed to clarify efficacy and safety in cesarean delivery. Cesarean delivery is among the most commonly performed surgical procedures worldwide 3 and is frequently associated with significant postoperative pain, which can negatively affect maternal recovery, breastfeeding, and early mother–newborn bonding 10. Strategies that safely reduce postoperative pain may improve obstetric outcomes.
Intraperitoneal local anesthetic administration has been evaluated as an adjunct for post-cesarean analgesia, but results remain heterogeneous and inconclusive 8 . The main objective of this study was to evaluate the efficacy and safety of intraperitoneal local anesthetic administration in reducing postoperative pain and side effects in women undergoing cesarean section, through a systematic review and meta-analysis of randomized controlled trials.
Methods
We conducted a systematic review and meta-analysis in accordance with PRISMA statement (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) and registered the protocol in PROSPERO (CRD 420251175263) (www.crd.york.ac.uk/Prospero). Planned analyses were performed as specified in the protocol. The research question was developed using the PICOS strategy (Population, Intervention, Comparison, Outcomes, Study design): Population (P): Women undergoing cesarean section; Intervention (I): Local anesthetics administered intraperitoneally; Comparison (C): Placebo, no intervention, or other analgesic techniques; Outcomes (O): Postoperative pain, analgesic consumption, postoperative nausea and vomiting, adverse events. The guiding question was: Does intraperitoneal local anesthetic administration reduce postoperative pain after cesarean section? The primary outcome was postoperative pain (intensity measured by the Visual Analog Scale (VAS) at 4, 6, 12 and 24 hours).
Secondary outcomes included postoperative nausea and vomiting (PONV), adverse effects within 24 hours, rescue opioid use within 24 hours, and patient satisfaction. The target population of the study included women undergoing cesarean delivery. We included randomized controlled trials (RCTs) evaluating intraperitoneal local anesthetic administration in women undergoing cesarean delivery and reporting postoperative pain and/or safety outcomes. Studies were eligible if published in English, Portuguese or Spanish. We excluded non-randomized studies, and obstetric procedures other than cesarean delivery. Searches were conducted in the following databases: PubMed, Embase, and Cochrane CENTRAL from January 1st, 1985 to January 15th, 2026. We used Boolean operators (AND/OR) and controlled vocabulary (e.g., MeSH) combined with keywords related to cesarean section, intraperitoneal administration, local anesthetics, and randomized trials.
The search included MeSH terms and keywords such as: ((randomized controlled trial[Publication Type] OR controlled clinical trial[Publication Type] OR randomized[Title/ Abstract] OR randomly[Title/Abstract] OR trial[Title/ Abstract] OR placebo[Title/Abstract]) NOT (animals[Mesh] NOT humans[Mesh])) AND (Cesarean Section[Mesh] OR cesarean[Title/Abstract] OR caesarean[Title/Abstract] OR cesarean delivery[Title/Abstract]) AND (intraperitoneal[Title/ Abstract] OR intra-peritoneal[Title/Abstract] OR peritoneal cavity[Title/Abstract]) AND (Anesthetics, Local[Mesh] OR "local anesthetic"[Title/Abstract] OR "local anesthesia"[Title/ Abstract] OR ropivacaine[Title/Abstract] OR bupivacaine[Title/ Abstract] OR lidocaine[Title/Abstract] OR mepivacaine[Title/ Abstract] OR prilocaine[Title/Abstract]) AND (Pain, Postoperative[Mesh] OR "postoperative pain"[Title/Abstract] OR "post-cesarean pain"[Title/Abstract] OR "postcesarean pain"[Title/Abstract] OR analgesia[Title/Abstract] OR analgesic[Title/Abstract]). Three independent reviewers screened titles, abstracts, and full texts identified by the bibliographic research. Data were extracted on: authors, year, country, number of participants, intervention characteristics, primary and secondary outcomes, main results, adverse events and risk of bias.
The PRISMA Flowchart was used as a standard for selecting the articles11. Grading of Recommendations Assessment, Development and Evaluation (GRADE) was applied. The risk of bias of the included studies was assessed using the Risk of Bias 2 (RoB 2) tool, developed by Cochrane for randomized clinical trials12. This tool considers five domains: (1) bias in the randomization process; (2) bias due to deviations from the intended intervention; (3) bias due to missing data; (4) bias in the measurement of outcomes; and (5) bias in the selection of reported results. Each study was assessed independently by two reviewers, with differences resolved by consensus or by a third reviewer. Judgments were categorized as “low risk of bias”, “some concerns” or “high risk of bias”, according to the instrument's guidelines.
An overall judgment was assigned to each study based on the combination of the five domains. The results are presented as a table and visual graph using the robvis13 tool. We extracted the data from individual studies using a 95% confidence interval. For binary endpoints the number of events was extracted and weighted mean differences were used to pool continuous outcomes. Heterogeneity was evaluated with Cochran Q test and I² statistics; p values inferior to 0.10 and I²>50% were considered significant for heterogeneity. DerSimonian and Laird random-effects model were used. Review Manager (RevMan) was used for statistical analysis.
Results
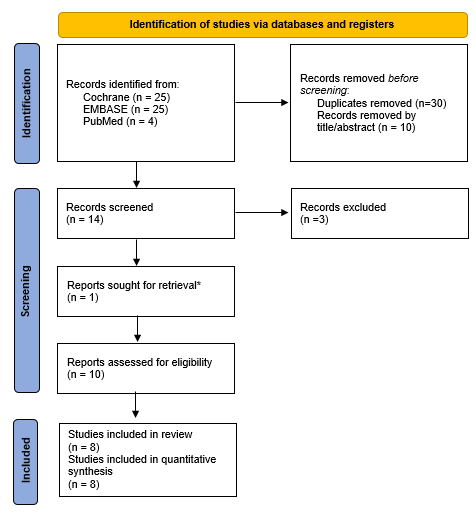
The electronic search results are described in detail in Figure 1, which shows a PRISMA diagram of our search and screening process. The electronic search and selection process is summarized in Figure 1 (PRISMA flow diagram). A total of 1,220 women were included. Searches retrieved 54 records (Cochrane CENTRAL n=25, Embase n=25, PubMed n=4). After removing 30 duplicates, 24 records were screened by title/abstract and 10 were excluded, leaving 14 reports for full-text assessment. Four full texts could not be retrieved. Ultimately, 10 randomized trials were included in the systematic review and meta-analysis. Nine trials evaluated elective cesarean delivery under spinal anesthesia; one trial used general anesthesia. Five studies used lidocaine, two used ropivacaine, and two used a lidocaine–bupivacaine mixture.
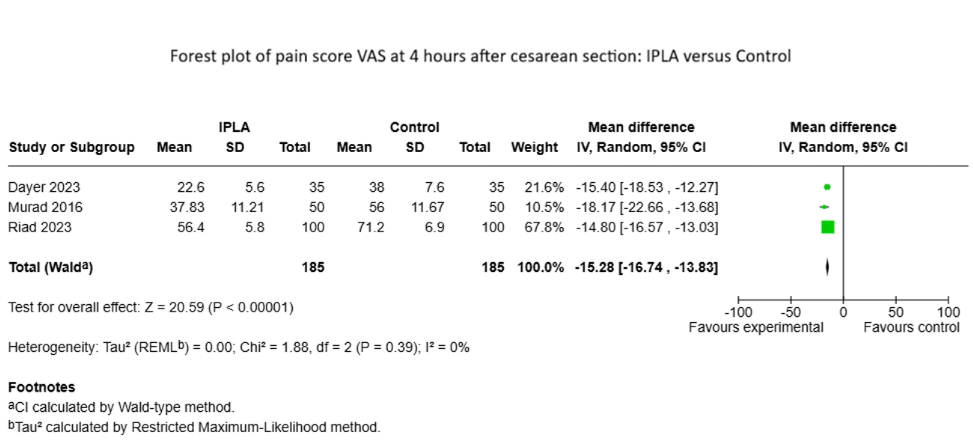
Instilled volumes ranged from 5 mL to 1.75 ml.kg-1 across studies. Grading of Recommendations Assessment, Development and Evaluation (GRADE) classified low certainty for the most part of outcomes. Postoperative nausea and vomiting demonstrate high certainty. VAS at 4 hours and side effects showed moderate certainty. The primary endpoint was analyzed by Visual Analogic Scale (VAS) (0-100) at 4, 6, 12 and 24 hours after the cesarean section. The VAS at 4 hours had a reduction of 15.28 points in favors to intraperitoneal local anesthetic with low heterogeneity (Tau2=0.0; p=0.39; I2=0%). VAS at 6, 12 and 24 hours did not demonstrate differences between the groups and showed a high heterogeneity in this analysis.
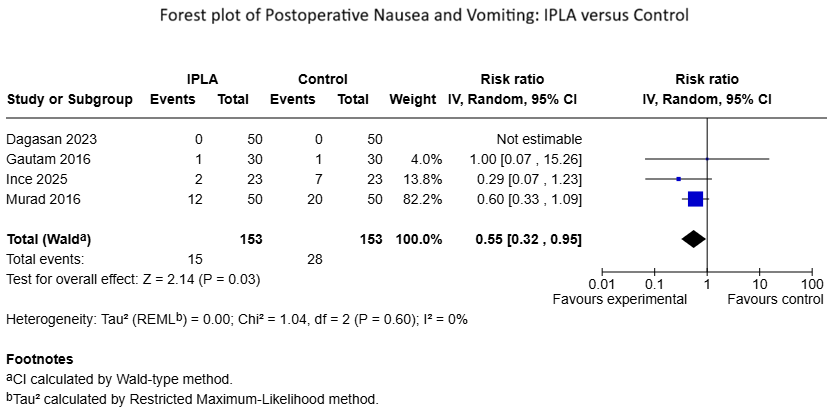
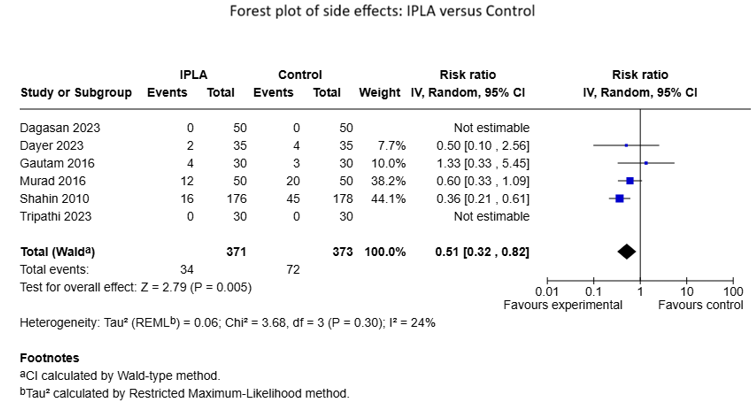
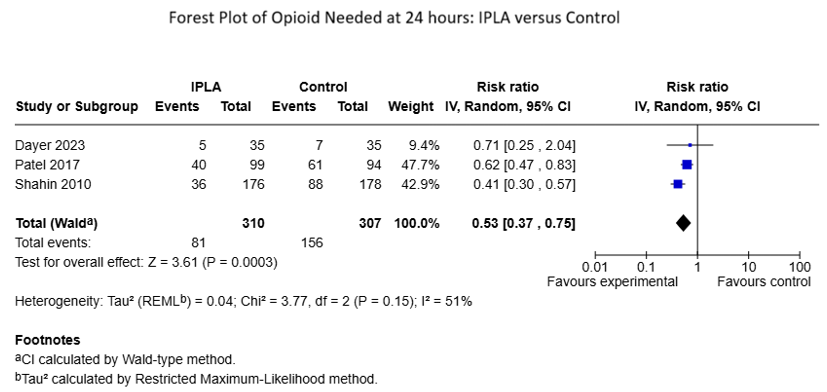
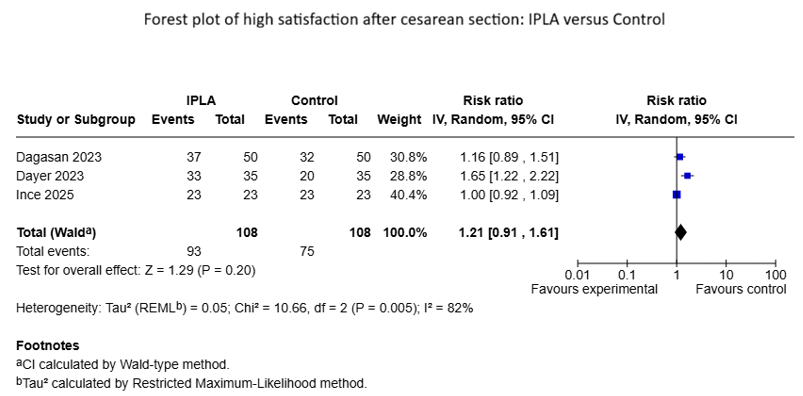
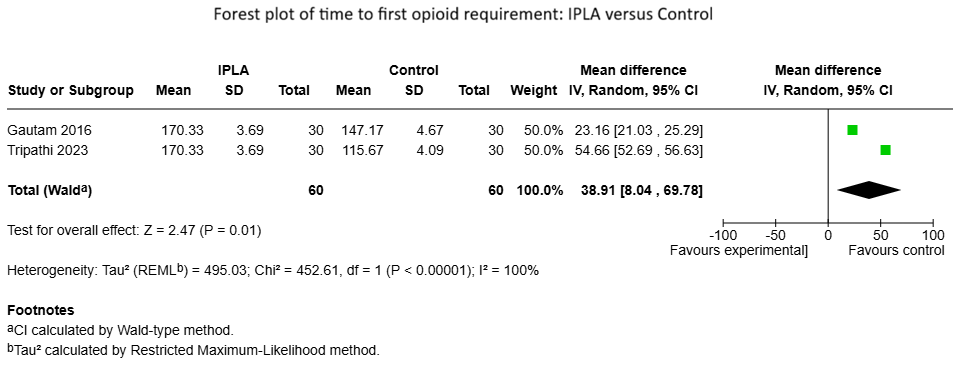
Secondary endpoints showed differences between the groups as described as follow. Postoperative nausea and vomiting (PONV) showed a reduction of 45% in favors to intervention group, with low heterogeneity (Tau2=0.0; p=0.59; I2=0%). Side effects showed almost half reduction to IPLA group with low heterogeneity (RR=0.51; Tau2=0.04; p=0.30; I2=19%). Opioid need at 24 hours had a 47% reduction to IPLA group with moderate heterogeneity (Tau2=0.04; p=0.14; I2=49%). Other endpoints as satisfaction (p<0.0001; I2=93%) and time to first opioid rescue (p<0.0001; I2=100%) showed high heterogeneity and no differences between the groups.
Discussion
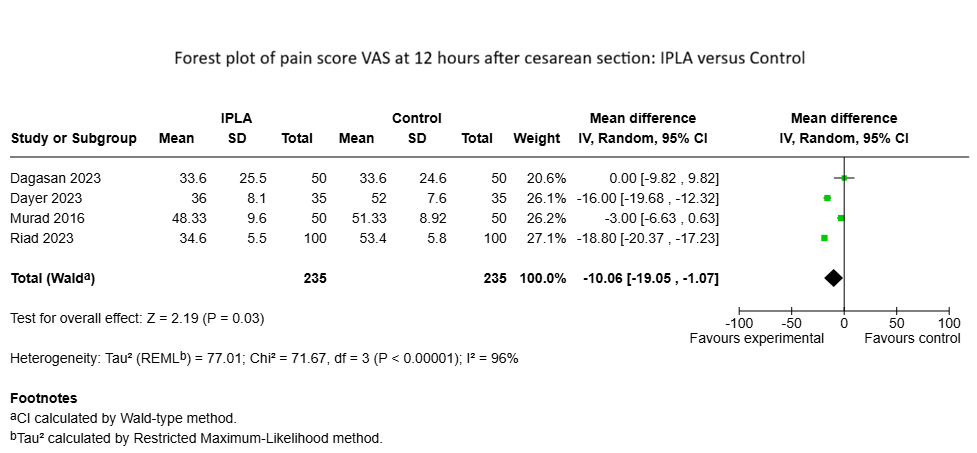
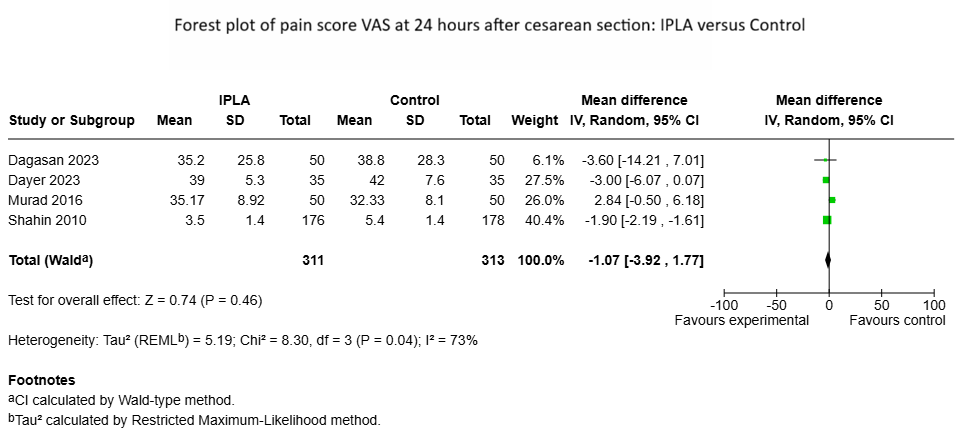
In this systematic review and meta-analysis, intraperitoneal local anesthetic administration (IPLA) during cesarean delivery was associated with meaningful improvements in early postoperative outcomes. The most consistent analgesic effect was observed at 4 hours, with a statistically significant reduction in pain and no heterogeneity, supporting a reproducible early analgesic benefit14–16 . At 6 hours, pooled pain scores continued to favor IPLA; however, between-study inconsistency was substantial (I²=93%), indicating that the magnitude of effect is strongly influenced by trial-level clinical and methodological differences14–16 .At12hours,thepooledestimatestillsuggested lower pain with IPLA (p=0.02), but heterogeneity was extreme (I²=96%), limiting confidence in the generalizability of the effect14–17 . By 24 hours, the pooled effect was small and not statistically significant, with moderate heterogeneity, suggesting uncertain durability of analgesic benefit beyond the early postoperative window14,15,17,18 .
Beyond pain scores, IPLA reduced the proportion of women requiring rescue opioids within 24 hours, suggesting a clinically relevant opioid-sparing effect14,18,19 . Consistent with reduced opioid exposure, IPLA was also associated with lower rates of postoperative nausea and vomiting (RR 0.55; I²=0%)15,17,20,21 and fewer reported side effects (RR 0.51; I²=19%)14,15,17,18,20,22 . Patient satisfaction did not show a clear improvement and exhibited marked heterogeneity, likely reflecting variability in measurement methods, timing, and co-interventions14,17,21 . Time to first rescue analgesia was longer with IPLA, but this outcome was based on few studies and showed extreme heterogeneity, limiting confidence in the pooled estimate. The temporal pattern of effects showed stronger and more consistent reduction in pain at 4 hours, with less consistent effects thereafter appears biologically plausible.
The most chosen local anesthetic among included studies was short action lidocaine. Early post-cesarean pain includes a visceral and peritoneal component related to tissue handling and peritoneal irritation; therefore, bathing the peritoneal cavity with local anesthetic may attenuate nociceptive input shortly after surgery23,24 . The heterogeneity in different dose, volume and not used adjuvants may contribute to the small effect on pain after 12 and 24 hours. As time progresses, the contribution of incisional/somatic pain, mobilization-related discomfort, and differences in scheduled multimodal analgesia may increase, potentially diluting the measurable incremental benefit of IPLA beyond the early postoperative period. The consistent reduction in rescue opioid requirement, along with lower PONV and fewer side effects, supports a clinically meaningful opioidsparing profile.
These benefits may be especially relevant in postpartum recovery, where minimizing opioid exposure can facilitate early mobilization and maternal–newborn interaction18,22–24 . Substantial heterogeneity in pain outcomes at 6 to 24 hours was expected because included trials varied in several effectmodifying domains. First of all, variation in local anesthetic agent, concentration, total dose, instilled volume, distribution within the cavity, and timing (e.g., before vs after peritoneal closure) likely influences exposure time and washout, generating heterogeneous effect sizes15,17,18,22 . Other factors that contribute to heterogeneous effects on follow up include baseline analgesic regimen and neuraxial opioid use: differences in intrathecal morphine use, systemic analgesics and multimodal scheduling can create ceiling effects, reducing the room for IPLA to demonstrate incremental analgesia and increasing variability between trials14,18,19,23 .
The outcomes measurements also could be influenced by cultural aspects related to pain. Pain was assessed using different scales and time points, and potentially at rest vs movement, which further inflates among-studies variability. Overall, side effects were lower with IPLA, likely reflecting reducedopioidexposureratherthandirectdrug-relatedharm. However, adverse event definitions were not standardized and rare complications may be under-detected in small trials. Future studies should systematically capture adverse events and report total local anesthetic dose (including neuraxial and wound components), with attention to toxicity monitoring25 . Trial sequential analysis (TSA) is particularly useful in metaanalyses with sparse data to explore the risk of random errors. In the present review, TSA could help differentiate outcomes that appear robust (low heterogeneity with significant pooled effects) from outcomes that remain inconclusive due to heterogeneity and limited information size.
Our sensitivity approach (e.g., excluding a clinically divergent trial such as Ince) reducing heterogeneity in some analyses is consistent with the interpretation that protocollevel differences, rather than random error alone, are major drivers of inconsistency21,26 . Strengths of this first meta-analysis about IPLA in cesarean include inclusion of randomized trials and assessment of clinically relevant endpoints (pain intensity, opioid rescue, PONV, adverse effects), as well as sensitivity considerations addressing heterogeneity. Limitations include the small number of trials per outcome, variability in IPLA protocols and co-interventions, and substantial heterogeneity in pain outcomes at more than 6 hours, which reduces confidence in the generalizability of later pain effects. Satisfaction was inconsistently measured and highly heterogeneous, limiting interpretability.
Accordingly, the most defensible conclusion is that IPLA offers reliable early analgesic benefit, while later analgesic effects are uncertain and context-dependent, particularly when background analgesia differs substantially across trials. IPLA is a simple and low-cost adjunct that appears most useful for improving early postoperative recovery-reducing pain at 4 hours and decreasing opioid rescue needs, with accompanying reductions in PONV and side effects. However, durability of analgesic benefit beyond the early postoperative window remains uncertain and likely contingent upon cointerventions and technique. Future trials should standardize multimodal analgesia, predefine pain assessment time points (rest and movement), and test optimized IPLA regimens (agent/dose/volume/timing), ideally stratified by intrathecal morphine use and incorporating patient-centered outcomes.
Abbreviations section PRISMA statement - Preferred Reporting Items for Systematic Reviews and Meta-Analysis GRADE - Grading of Recommendations Assessment, Development and Evaluation randomized controlled trials (RCTs) Visual Analog Scale (VAS) postoperative nausea and vomiting (PONV) Declarations Ethics Approval – not applicable Consent for Participation and Publication – not applicable Availability of data and materials – we collected data from articles published. All data are available in Excel plan Competing interests – no conflict of interests Funding – no funding Authors' contributions (individual contributions using initials. JCR provided the design, articles found, classifying articles, data analysis, write the first and final version. TRE provided articles found, data analysis, write versions. JCMB provided the design, articles found, classifying articles, data analysis, write the first and final versions.
CSG provided classifying articles, data analysis, write paper versions. TMS was responsible for all steps in this research) Acknowledgements - none Clinical Trial Registration - PROSPERO (CRD 420251175263) Table 1. Baseline characteristics of local anesthetic administration’s use after cesarean section. Authors/ Year Country Study design Intervention /Control (N) Age Type of cesarean section Type of anesthesia Intervention Time of Administration Follow up duration Shahin & Osman, 2010 Egypt RCT 370 (185/185) Lidocaine: 25,3 +/- 6,8 SD. Control: 26,2 +/- 5,2 SD. Elective General anesthesia IP instillation After uterine closure, before peritoneal closure. 8 months Murad et al., 2016 Egypt RCT- 3 arms 100 (50/50) IP group: 27,88 +/- 4,53 SD..
Control: 27,82 +/- 4,41 SD. Elective Subarachnoid anesthesia IP instillation X IV instillation IP after closing uterine incision and before parietal peritoneal closure VS. IV Bolus at induction + continuous infusion 24 hours Gautan et al., 2016. India RCT -3 arms 90 (30/30/30) G1: 24.37 +/- 3.65. G2: 26.5 +/- 5.871. G3: 25.1 +/- 4.4. Elective Subarachnoid anesthesia local infiltration of 20mL ropivacaine 0,2% at incision site VS. LI 15mL ropivacaine 0,2% at the incision site and IP instillation of 5mL ropivacaine 0,2%. Before closure of peritoneum Not specified Patel et al., 2017 USA RCT 204 (99/94) Lidocaine: 35,1 +/- 4,1 SD. Placebo: 35,6 +/- 4,3 SD Elective Subarachnoid anesthesia IP instillation Before paritoneal peritoneum or fascia closure 48 hours Riad et al., 2023 Egypt RCT 200 (100/100) Lidocaine: 28,4 +/- 5,8 SD.
Control: 28,9 +/- 6,2 SD. Not specified Subarachnoid anesthesia IP instillation After uterine closure, before peritoneal closure, 5mL of the drug onto each quadrant of the uterus. 12 hours Dagasan- Cetin et al., 2022 Turkey RCT -3 arms 150 (50/50/50) LWI: 29,1 +/- 5,61 SD // 28 (20-41). IPLA: 30,2 +/- 5,61 SD // 29 (20-43). Placebo: 31,76 +/- 5,08 SD // 31,5 (24-50). Elective Subarachnoid anesthesia IP instillation X Local infiltration Subcutaneous: at the end of surgery prior to skin closure. IP: before fascia closure 24 hours Dayer et al., 2023 Egypt RCT 70 (35/35). Lidocaine: 23,9 +/- 1,8 SD // 21-28. Placebo: 24,1 +/- 1,8 SD // 21-28 Elective Subarachnoid anesthesia IP instillation Before closing the parietal peritoneum or fascia.
24 hours Ince et al., 2025 Turkey RCT 46 (23/23) Group M: 29,65 +/- 4,62 SD // 29 (22- 40). Group LWI + RAI + IPLA: 30,6 +/- 5,36 SD // 29 (20-41). Elective Subarachnoid anesthesia 15mL of bupivacaine 0,5% + 15mL de lidocaine 2% + 1:200.000 epinefrin: 10mL intraperitoneal, 10mL infiltration in rectus aponeurosis and 10mL at the incision site Before closure of peritoneum 24 hours Data presented as: *RCT: randomized controlled trial; †Mean±SD; ‡Number (n); SD=Standard deviation, ASA=American Society of Anesthesiologists; BMI=Body mass index; VAS= Visual Analog Scale; + = (IQR )Median Interquartile range; ~ = frequency (%), LWI: Light Well Intervention, R1/R2: Ropivacaine ½, NRSs: Numerical Rating Scale.
GRADE IPLA. cesarean section. Outcome Number of Studies Study Design Risk of Bias (RoB) Indirect Evidence Imprecision Funnel Plot (Publication Bias) Overall Certainty of Evidence Absolut risk IPLA Rate / Effect (95% CI) VAS Pain Score at 4 hours N = 370 (3 RCTs) RCT Not serious Not serious Not serious (I²=0%; Tau²=0.0) Less than 10 studies Moderate MD -15.28 MD −15.28 (−16.74 to −13.83) Favors IPLA VAS Pain Score at 6 hours N = 185 (3 RCTs) RCT Not serious Not serious Serious (I²=93%; Tau²=46.34) Less than 10 studies Low MD-11.32 MD −11.32 (−19.38 to −3.27) Favors IPLA VAS Pain Score at 12 hours N = 235 (4 RCTs) RCT Not serious Not serious Serious (I²=96%; Tau²=70.11) Less than 10 studies Low MD -10.11 MD −10.11 (−18.72 to −1.50) Favors IPLA VAS Pain Score at 24 hours N = 313 (4 RCTs) RCT Not serious Not serious Serious (I²=64%; Tau²=3.41) Less than 10 studies Low MD -1.11 MD −1.11 (−3.55 to +1.32) Favors IPLA Satisfaction N = 108 (3 RCTs) RCT Not serious Not serious Serious (I²=93%; Tau²=0.16) Less than 10 studies Low RAR 16.7% RR 1.23 (0.77 to 1.97) Favors IPLA Postoperative Nausea and V o m i t i n g (PONV) N = 306 (4 RCTs) RCT Not serious Not serious Not serious (I²=0%; Tau²=0.0) Less than 10 studies High 183 -> 101/1000 (18.3%) RR 0.55 (0.32 to 0.95) Favors IPLA Side Effects N = 744 (6 RCTs) RCT Not serious Not serious Not serious (I²=24%; low heterogeneity) Less than 10 studies Moderate 193 -> 98/1000 (19.3%) RR 0.51 (0.32 to 0.82) Favors IPLA Graphics and tables Figure 1.
PRISMA 2020 flow diagram for new systematic reviews. Figure 2. Risk of Bias Figure 3. VAS 4h Figure 4. VAS 6h Figure 5. VAS 12h Figure 6. VAS 24h. Figure 7. PONV Figure 8. side effects Figure 9. opioids needed 24h Figure 10. satisfaction Figure 11. 1st time opioid rescue
Figures and Tables


| Authors/ Year | Country | Study design | Intervention /Control (N) | Age | Type of cesarean section | Type of anesthesia | Intervention | Time of Administration | Follow up duration |
|---|---|---|---|---|---|---|---|---|---|
| Shahin & Osman, 2010 | Egypt | RCT | 370 (185/185) | Lidocaine: 25,3 +/- 6,8 SD. Control: 26,2 +/- 5,2 SD. | Elective | General anesthesia | IP instillation | After uterine closure, before peritoneal closure. | 8 months |
| Murad et al., 2016 | Egypt | RCT- 3 arms | 100 (50/50) | IP group: 27,88 +/- 4,53 SD.. Control: 27,82 +/- 4,41 SD. | Elective | Subarachnoid anesthesia | IP instillation X IV instillation | IP after closing uterine incision and before parietal peritoneal closure VS. IV Bolus at induction + continuous infusion | 24 hours |
| Gautan et al., 2016. | India | RCT -3 arms | 90 (30/30/30) | G1: 24.37 +/- 3.65. G2: 26.5 +/- 5.871. G3: 25.1 +/- 4.4. | Elective | Subarachnoid anesthesia | local infiltration of 20mL ropivacaine 0,2% at incision site VS. LI 15mL ropivacaine 0,2% at the incision site and IP instillation of 5mL ropivacaine 0,2%. | Before closure of peritoneum | Not specified |
| Patel et al., 2017 | USA | RCT | 204 (99/94) | Lidocaine: 35,1 +/- 4,1 SD. Placebo: 35,6 +/- 4,3 SD | Elective | Subarachnoid anesthesia | IP instillation | Before paritoneal peritoneum or fascia closure | 48 hours |
| Riad et al., 2023 | Egypt | RCT | 200 (100/100) | Lidocaine: 28,4 +/- 5,8 SD. Control: 28,9 +/- 6,2 SD. | Not specified | Subarachnoid anesthesia | IP instillation | After uterine closure, before peritoneal closure, 5mL of the drug onto each quadrant of the uterus. | 12 hours |
| Dagasan- Cetin et al., 2022 | Turkey | RCT -3 arms | 150 (50/50/50) | LWI: 29,1 +/- 5,61 SD // 28 (20-41). IPLA: 30,2 +/- 5,61 SD // 29 (20-43). Placebo: 31,76 +/- 5,08 SD // 31,5 (24-50). | Elective | Subarachnoid anesthesia | IP instillation X Local infiltration | Subcutaneous: at the end of surgery prior to skin closure. IP: before fascia closure | 24 hours |
| Dayer et al., 2023 | Egypt | RCT | 70 (35/35). | Lidocaine: 23,9 +/- 1,8 SD // 21-28. Placebo: 24,1 +/- 1,8 SD // 21-28 | Elective | Subarachnoid anesthesia | IP instillation | Before closing the parietal peritoneum or fascia. | 24 hours |
|---|---|---|---|---|---|---|---|---|---|
| Ince et al., 2025 | Turkey | RCT | 46 (23/23) | Group M: 29,65 +/- 4,62 SD // 29 (22- 40). Group LWI + RAI + IPLA: 30,6 +/- 5,36 SD // 29 (20-41). | Elective | Subarachnoid anesthesia | 15mL of bupivacaine 0,5% + 15mL de lidocaine 2% + 1:200.000 epinefrin: 10mL intraperitoneal, 10mL infiltration in rectus aponeurosis and 10mL at the incision site | Before closure of peritoneum | 24 hours |
| Outcome | Number of Studies | Study Design | Risk of Bias (RoB) | Indirect Evidence | Imprecision | Funnel Plot (Publication Bias) | Overall Certainty of Evidence | Absolut risk | IPLA Rate / Effect (95% CI) |
|---|---|---|---|---|---|---|---|---|---|
| VAS Pain Score at 4 hours | N = 370 (3 RCTs) | RCT | Not serious | Not serious | Not serious (I²=0%; Tau²=0.0) | Less than 10 studies | Moderate | MD -15.28 | MD −15.28 (−16.74 to −13.83) Favors IPLA |
| VAS Pain Score at 6 hours | N = 185 (3 RCTs) | RCT | Not serious | Not serious | Serious (I²=93%; Tau²=46.34) | Less than 10 studies | Low | MD-11.32 | MD −11.32 (−19.38 to −3.27) Favors IPLA |
| VAS Pain Score at 12 hours | N = 235 (4 RCTs) | RCT | Not serious | Not serious | Serious (I²=96%; Tau²=70.11) | Less than 10 studies | Low | MD -10.11 | MD −10.11 (−18.72 to −1.50) Favors IPLA |
| VAS Pain Score at 24 hours | N = 313 (4 RCTs) | RCT | Not serious | Not serious | Serious (I²=64%; Tau²=3.41) | Less than 10 studies | Low | MD -1.11 | MD −1.11 (−3.55 to +1.32) Favors IPLA |
| Satisfaction | N = 108 (3 RCTs) | RCT | Not serious | Not serious | Serious (I²=93%; Tau²=0.16) | Less than 10 studies | Low | RAR 16.7% | RR 1.23 (0.77 to 1.97) Favors IPLA |
| Postoperative Nausea and Vomiting (PONV) | N = 306 (4 RCTs) | RCT | Not serious | Not serious | Not serious (I²=0%; Tau²=0.0) | Less than 10 studies | High | 183 -> 101/1000 (18.3%) | RR 0.55 (0.32 to 0.95) Favors IPLA |
| Side Effects | N = 744 (6 RCTs) | RCT | Not serious | Not serious | Not serious (I²=24%; low heterogeneity) | Less than 10 studies | Moderate | 193 -> 98/1000 (19.3%) | RR 0.51 (0.32 to 0.82) Favors IPLA |
References
- Betran AP, Ye J, Moller AB, Souza JP, Zhang J. Trends and projections of caesarean section rates: global and regional estimates. BMJ Glob Health. 2021 Jun;6(6):e005671.
- Weibel S, Neubert K, Jelting Y, Meissner W, Wöckel A, Roewer N, Kranke P. Incidence and severity of chronic pain after caesarean section. Eur J Anaesthesiol. 2016 Nov;33(11):853–865.
- Betrán AP, Ye J, Moller AB, Zhang J, Gülmezoglu AM, Torloni MR. The Increasing Trend in Caesarean Section Rates: Global, Regional and National Estimates: 1990- 2014. PLoS One. 2016 Feb 5;11(2):e0148343.
- Marzoni FS, Faramarzi M, Ghanbarpoor A, Seyfi S, Gholinia H, Abasabadi HR. Psychosocial Factors of Post-operative Pain Intensity in Women Undergoing Cesarean Section. Shiraz E Medical Journal. Brieflands; 2022 Jul 1;23(7).
- Hawkins JL. Anesthesia-Related Maternal Mortality. Clin Obstet Gynecol. 2003 Sep;46(3):679–687.
- Eisenach JC, Pan PH, Smiley R, Lavand’homme P, Landau R, Houle TT. Severity of acute pain after childbirth, but not type of delivery, predicts persistent pain and postpartumdepression.Pain.2008Nov15;140(1):87–94.
- Sultan P, Halpern SH, Pushpanathan E, Patel S, Carvalho B. The Effect of Intrathecal Morphine Dose on Outcomes After Elective Cesarean Delivery: A Meta-Analysis. Anesth Analg. 2016 Jul;123(1):154–164.
- Boulianne M, Verret M, O’Connor S, Savard X, Neveu X, Marcoux C, Costerousse O, Gagnon MA, Zhang H, Beaulé L, Lamothe-Boucher F, Turgeon AF. Intraperitoneal local anestheticsforpostoperativepainmanagementfollowing intra-abdominal surgery: a systematic review and metaanalysis. BMC Anesthesiol. 2025 May 10;25(1):235.
- Marchand G, Ware K, Govindan M, Masoud AT, King A, Ruther S, Brazil G, Cieminski K, Calteux N, Coriell C, Ulibarri H, Parise J, Arroyo A, Chen D, Pierson M, Rafie R, Sainz K. A Systematic Review and Meta-Analysis of Intraperitoneal Bupivacaine in Laparoscopic Gynecologic Surgery. J Pain Res. 2021 Sep;Volume 14:2699–2707.
- Karlström A, Engström-Olofsson R, Norbergh K, Sjöling M, Hildingsson I. Postoperative Pain After Cesarean Birth Affects Breastfeeding and Infant Care. Journal of Obstetric, Gynecologic & Neonatal Nursing. 2007 Sep;36(5):430–440.
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hróbjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, McGuinness LA, Stewart LA, Thomas J, Tricco AC, Welch VA, Whiting P, Moher D. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021 Mar 29;n71.
- Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, Cates CJ, Cheng HY, Corbett MS, Eldridge SM, Emberson JR, Hernán MA, Hopewell S, Hróbjartsson A, Junqueira DR, Jüni P, Kirkham JJ, Lasserson T, Li T, McAleenan A, Reeves BC, Shepperd S, Shrier I, Stewart LA, Tilling K, White IR, Whiting PF, Higgins JPT. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019 Aug 28;l4898.
- McGuinness LA, Higgins JPT. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res Synth Methods. 2021 Jan 6;12(1):55–61.
- Dayer MZS, Salama HFM, Anter ME. Intraperitoneal Lidocaine Instillation for Postoperative Pain Relief after Cesarean Delivery [Internet]. The Egyptian Journal of Hospital Medicine. 2023 Oct. Available from: https:// ejhm.journals.ekb.eg/
- Anwar Murad AW, Elhadi Farag MA, Abosrie M, Abd Alazeem ES, Mostafa A. Efficacy of intraperitoneal versus intravenous lidocaine for postcesarean pain relief. Evidence Based Womenʼs Health Journal. Ovid Technologies (Wolters Kluwer Health); 2016 Nov;6(4):144–148.
- Riad A, Taha M, Hamza SHM, Abdelhamed AM. Efficacy of intraperitoneal Lidocaine for post cesarean section Analgesia: A prospective randomized, doubleblind, placebo-controlled clinical trial. Ginekologia i położnictwo. 2023 Mar 29;18(1):1–5.
- Dagasan Cetin G, Dostbil A, Aksoy M, Kasali K, Ince R, Kahramanlar AA, Atalay C, Topdagi Yilmaz EP, Ince I, Ozkal MS. Intraperitoneal instillation versus wound infiltration for postoperative pain relief after cesarean delivery: A prospective, randomized, double-blind, placebo-controlled trial. Journal of Obstetrics and Gynaecology Research. John Wiley and Sons Inc; 2023 Jan 1;49(1):209–219. PMID: 36270632
- Shahin AY, Osman AM. Intraperitoneal Lidocaine Instillation and Postcesarean Pain After Parietal Peritoneal Closure A Randomized Double Blind Placebocontrolled Trial [Internet]. 2010. Available from: www. clinicalpain.com
- Patel R, Carvalho JCA, Downey K, Kanczuk M, Bernstein P, Siddiqui N. Intraperitoneal instillation of lidocaine improves postoperative analgesia at cesarean delivery: A randomized, double-blind, placebo-controlled trial. Anesth Analg. Lippincott Williams and Wilkins; 2017. p. 554–559. PMID: 27984226
- Gautam A, Muzalda B, Tandon N. Ropivacaine hydrochloride 0.2% local infiltration and intraperitoneal instillation for postoperative pain relief in cesarean section under spinal anaesthesia: a randomised clinical study. J Evol Med Dent Sci. Akshantala Enterprises Private Limited; 2016 Sep 29;5(78):5816–5819.
- Ince R, Yilmaz MA, Ozkal Yalin MS, Dostbil A, Kasali K, Cimilli Senocak GN, Aksoy M, Tapanoglu Karaca S, Ince I, Atalay C. Comparison of the Efficacy of Postcesarean Analgesia by Combination of Intraperitoneal Instillation of Local Anaesthetics, Rectus Aponeurosis Infiltration and Infiltration Through the Wound Site Versus Intratechal Morphine: Prospective, Randomised, Double-Blind Study [Internet]. 2025. Available from: https://www.preprints.org/manuscript/202503.1176/v1
- Tripathi S, Thakre S, Narrey N, Dandotiya D, Singh P, Jain AK. A comparison of post-operative pain relief after elective LSCS with local and intraperitoneal ropivacaine instillation against local ropivacaine infiltration alone. Asian Journal of Pharmaceutical and Clinical Research. 2023 Apr 7;18–20.
- Veef E, Van de Velde M. Post-cesarean section analgesia. Best Pract Res Clin Anaesthesiol. 2022 May;36(1):83–88.
- Meyer MF, Broman AT, Gnadt SE, Sharma S, Antony KM. A standardized post-cesarean analgesia regimen reduces postpartum opioid use. The Journal of Maternal-Fetal & Neonatal Medicine. 2022 Dec 12;35(25):8267–8274.
- Becker DE, Reed KL. Local Anesthetics: Review of Pharmacological Considerations. Anesth Prog. 2012;59(2):90–102.
- Masoumeh S, Valami H, Abbas S, Jahromi H, Mahmoodi T, Barikani A. Comparing the Effects of Intraperitoneal InjectionofBupivacaine,Morphine,andDexamethasone on Pain after Elective Caesarean Section under General Anesthesia. 2017.
This is a text version generated from the article. For the formatted version of record (with original tables & figures), download the PDF →