Full Text Hide / show
Background
: Diabetes is a chronic disorder caused by elevated levels of blood glucose or insulin hormone deficiency. Diabetes is a common chronic illness and it is linked with a high rate of morbidity and mortality. Diabetes mellitus (DM) therapy is mostly dependent on patients’ ability to self-care in their daily lives; hence the knowledge, attitude and practices (KAP) of a diabetic patient is generally regarded a vital component of DM management. Objective: To assess the impact of basic diabetes literacy on daily self-management practices among type 2 diabetes patients. Materials and Methods:The study used cross-sectional design where 120 participants were recruited. Data on socio-demographic characteristics, medical history, knowledge on diabetes and self-care practices were collected and analysed using SPSS version 25.
Results
were presented using descriptive, inferential, percentages and chi- square. Results: The study recruited 120 participants where 102 (85%) were females and 18(15%) were males. Assessing educational level, 55.8 % of the participants attaining Junior High School level of education. About 51.7% of the participants had adequate knowledge when asked about the signs and symptoms of high blood sugar. Alarmingly, 84% of the participants were ignorant of the fact that a diabetic must check his or her feet regularly. Most of the participants (60%) had no knowledge about the normal fasting blood glucose level and 93.3 % either had no knowledge or inadequate knowledge about how often a diabetic should exercise.
97% and 96% of the participants failed to regularly check their blood pressure and glucose level respectively. Also, the study noted that, 83% and 89% exhibited poor self-care practices such as checking their feet regularly and visiting the eye doctor respectively. The study recommends that in order to improve disease management outcomes, healthcare workers intensify education on self-care management Conclusion and implication: The study recommends that in order to improve disease management outcomes, healthcare workers intensify education on self-care management. Keywords: basic diabetes literacy, daily self-management, practices, type 2 diabetes patients.
Introduction
Diabetes has emerged as a major public health concern globally. In 2017, approximately over 451 million individuals globally were diagnosed with diabetes. This figure is expected to accelerate to 693 million by 2045 according to International Diabetes Federation (1,2). Currently, 19 million adults in Africa have diabetes which is expected to rise to 47 million by 2045 (3,4). According to 5[5] 24 million people were living with diabetes in sub-Saharan Africa as of 2021 and the projected figure is likely to be 100% by 2045. Presenting the assertions further, WHO, reports that, Type 2 diabetes accounts for 90-95 percent of all diabetes cases worldwide (6). In Ghana, 2.4 million diabetics have been recorded with 5.3% of them having adult Type-2 Diabetes (7).
The motivation to control this surge is partly based on early awareness and adequate knowledge of diabetes management practices among diabetic patients. However, available research reports reveal that 69.2% of adults are unaware of their disease condition (3,4). High rates of undiagnosed diabetes mean that a significant portion of the population is likely living with chronic hyperglycaemia for years before diagnosis. This allows diabetes-related complications such as retinopathy, neuropathy, kidney failure, and cardiovascular disease to develop and worsen silently (8). Again, unaware individuals cannot take proactive steps to manage their health, resulting in higher rates of morbidity and mortality. In addition, lack of awareness may perpetuate the epidemic, as individuals may continue unhealthy dietary habits and sedentary lifestyles, unknowingly accelerating the disease progression (9,10).
Equally, patients who are diagnosed, but have limited knowledge regarding diabetes management practices may be implicated in poor glycaemic control, further increasing the risk of acute emergencies like hypoglycaemia or diabetic ketoacidosis (11 ,12,13). Examining this gamut of health risks present fertile grounds to assess the knowledge and management practices of diabetic patients in Ghana. Aside medication, many research outcomes have established that, effective DM management essentially depends on patients’ basic knowledge and ability to self-care. Basic knowledge of diabetes improves care practices by enabling patients and healthcare providers to adopt more effective selfmanagement strategies, resulting in better glyceamic control, fewer complications, and increased treatment adherence. Understanding the disease allows for necessary lifestyle modifications (diet and exercise), consistent monitoring, and proactive prevention of complications (14).
Equally, self-care practices including diet, exercise, medication adherence, and blood sugar monitoring significantly improve glycemic control (lower levels), enhance insulin sensitivity, maintain target glucose levels, and improve overall quality of life (15,16,17.18) Diabetes knowledge and self-care among Ghanaians with Type 2 diabetes is generally poor, with nearly 47% showing limited understanding of the condition. While medication adherence is moderate (33.5–84.5%), self-management behaviours like blood glucose monitoring (0.5–2.2 days/ week) and foot care are suboptimal. Key challenges include limited specialized care and, for many, a reliance on general advice rather than personalized education (19,20,21) Other publications have revealed that, in Ghana, most people (with or without the disease) are unaware of the causes and complications of the disease and how to successfully manage the condition (22, 23).
This could be attributed to low literacy rate of diabetes. According to (24) diabetic patients with low literacy may be at higher risk of poor health outcomes. Also, a study by (25, 26) noted that improving patient knowledge of diabetes mellitus and its consequences improves patient compliance with treatment, perhaps leading to a reduction in complications. In Ghana, a lot of initiatives have been adopted nationally to help improve knowledge, attitude, and practices of diabetic patients (1). Despite these national interventions, there is paucity of information on status of basic knowledge and selfcare practices among diabetic patients visiting the diabetic clinic at the Ejisu Government Hospital in Ghana. This study therefore seeks to assess the impact of basic diabetes literacy on daily self-management practices among type 2 diabetes patients in Ejisu municipality of Ghana
Materials and Methods
Study design and approach The study was a cross-sectional study with quantitative approach. A cross-sectional study with a quantitative approach is highly suitable for assessing the knowledge and self-care practices of diabetic patients because it offers an efficient, cost-effective way to measure the prevalence of specific health behaviours and knowledge gaps within a large population at a single point in time. This research design and approach allow for the statistical analysis of relationships between sociodemographic factors (like education or age) and self-care behaviours, such as diet, exercise, and blood glucose monitoring. Data collected through structured questionnaires, such as the summary of diabetes self-care activities, allows for standardized, objective-like, self-reported data that can be analyzed to evaluate how well patients manage their illness.
Study Population The study population were known diabetic patients accessing healthcare at Ejisu Government Hospital and Onwe Government Hospital in the Ejisu Municipality of Ghana. Inclusion criteria The inclusion criteria were patients, Ⅰ.who were 18 years and above. Ⅱ.who have been medically diagnosed with diabetes Ⅲ.Who frequently visited the Onwe and Ejisu Government Hospitals. Ⅳ.who consented to participate in the study. Exclusion criteria The exclusion criteria were patients; Ⅰ. Who were less than 18 years. Ⅱ.who did not consent to be participants Ⅲ. who had complicated health conditions with comorbidities Sampling size and technique Respondents were recruited by convenience from the Diabetic Clinics of Ejisu Government Hospital and Onwe Government Hospital.
Respondents who met the inclusion criteria (n=120) were recruited. Recruitment was based on definite clinical diagnosis of diabetes by qualified medical personnel. Formal introduction, intentions and consents were sought after which questionnaires were administered. Sample Size calculation To achieve an 80% power to detect a 1% difference in HbAlC, the sample size was determined using the formula of (27) as shown below: Where n is the sample size, μ_1refers to the population mean in the intervention group (HbAlC = 9.9), μ_2 is the population means in the control group (HbAlC = 8.9), a = 1.96 for alpha (0.05), b = 0.842 for power (0.80) and ǒ is the population standard deviation of 1.6.
The estimated sample size was 60. Therefore, 60 participants were recruited in each arm of the study. (control and interventional group). Data Collection tools The questionnaire used consisted of three sections. The first section covered questions on sociodemographic data. The second section covered questions relating to family and medical history. The third section covered questions relating to basic knowledge and basic daily practices of diabetic patients. The questions were adopted from (28). Ethical Consideration Ethical approval was sought from the Committee on Human Research, Publication and Ethics, School of Medical Sciences (CHRPE) of KNUST with the reference number (CHRPE/ RC/168/22). The participants were told the direct and indirect benefits of participating in the research.
They were not forced to take part in the study as participation was voluntary. They were also told they have the right to withdraw from the study at any time without any penalty. Also, they had the right not to answer any question they felt uncomfortable about. They were assured of confidentiality.
Results
Sociodemographic Characteristics of Study Participants The study included 120 participants, evenly distributed between Ejisu Government Hospital and Onwe Government Hospital, with each facility accounting for 50.0% of the total participants. The majority of the participants were aged 51 years and older (77.5%). Gender distribution showed that most participants were female (85.0%). The highest proportion of study participants were Akan (92.5%) and the least being Northerners (3.3%). Almost half of the participants were married (44.2%), while 30.8% were widowed, 16.7% divorced, and 8.3% single. Regarding education, 55.8% had completed JHS/MSLC, while 19.2% had no formal education. Religiously, the vast majority identified as Christians (95.0%), with a small percentage being Muslim (4.2%).
More than half of the participants (60.0%) were self-employed. Table 1 displays the sociodemographic characteristics of the study participants. Table 1. Sociodemographic Characteristics of Study Participants. Variable Frequency (n=120) Percentage (%) Facility Ejisu Government Hospital 60 50.0 Onwe Government Hospital 60 50.0 Age Group (Years) 18-40 6 5.0 41-50 21 17.5 ≥ 51 93 77.5 Gender Male 18 15.0 Female 102 85.0 Ethnicity Akan 111 92.5 Ewe 5 4.2 Northerner 4 3.3 Marital Status Single 10 8.3 Divorced 20 16.7 Widowed 37 30.8 Married 53 44.2 Educational Level No formal education 23 19.2 Primary 18 15.0 JHS/MSLC 67 55.8 SHS 4 3.3 Tertiary 8 6.7 Religious Affiliation Christian 114 95.0 Muslim 5 4.2 Traditionalist 1 0.7 Employment Status Unemployed 41 34.2 Self-employed 72 60.0 Employed 7 5.8 Note: Data presented as frequency and percentage.
Abbreviations: JHS: junior high school/ middle school leaving certificate; SHS: senior high school. Medical History and Clinical Characteristics of Study Participants Medical history and clinical characteristics of study participants is displayed in Table 2. A notable 66.7% of the participants reported having a family history of diabetes, with parents being the most commonly affected relatives (35.0%). Interestingly, 22.5% of those with a family history indicated that both their parents and siblings were affected. 40.0% of study participants lived with diabetes for six years or more while 39.2% for 2-5 years, and 20.8% for less than two years. Metformin was the most commonly used diabetes medication, with 69.2% of participants relying on it.
However, 27.5% of the participants were on a combination of metformin and glibenclamide with a very small percentage (0.8%) on insulin. Majority of participants (76.7%) had other non-communicable diseases (NCDs) with all participants with another NCD having hypertension. Table 2. Medical History and Clinical Characteristics of Study Participants. Variable Frequency (n=120) Percentage (%) Family History of Diabetes No 40 33.3 Yes 80 66.7 Specific Family Member (If Yes) Parent 28 35.0 Siblings 22 27.5 Grandparents 1 1.3 Uncle 4 5.0 Auntie 7 8.8 Parent and Siblings 18 22.5 Duration of Diabetes (Years) < 2 25 20.8 2-5 47 39.2 ≥ 6 48 40.0 Diabete Drugs Metformin 83 69.2 Glibernclamide 3 2.5 Metformin and glibenclamide 33 27.5 Insulin 1 0.8 Do you have any other NCDs No 28 23.3 Yes 92 76.7 Specific Other NCD (If Yes) Hypertension 92 100.0 Data presented as frequency and percentage.
NCDs: non-communicable diseases Knowledge Level on Diabetes Among Study Participants A significant number of participants (53.3%) recognized frequent urination as a symptom of hyperglycaemia, with 45.0% identifying extreme thirst. However, awareness of symptoms like blurred vision (32.5%) and tiredness/fatigue (31.7%) was lower. A worrying 65.8% of participants admitted they didn’t know how to treat hypoglycaemia, while only 21.7% mentioned using juice or soft drinks like Coke or Fanta, and 12.5% suggested hard candy or sweets as a treatment method. Foot care is grossly neglected, with 71.1% of participants not checking their feet at all. Furthermore, 80.8% didn’t understand the importance of foot checks in preventing neuropathy-related complications. Eye health was also under-prioritized, with 85.8% of participants only seeing an eye doctor when necessary, and only 14.2% having an annual eye check-up.
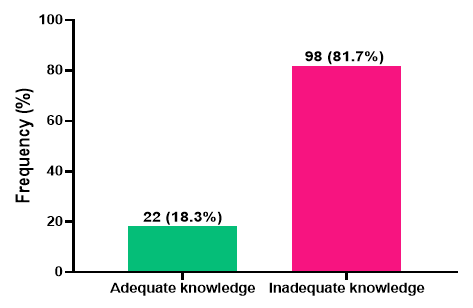
Knowledge about normal blood glucose levels and HbA1C ranges was shockingly low, with 60.0% and 94.2% of participants, respectively, unable to identify the correct ranges. Regarding the long-term complications of diabetes, while 45.0% of participants were aware of the risk of blindness, fewer recognized the dangers of cardiovascular disease (40.8%) or amputation (26.7%). Almost all study participants (99.2%) did not recognize the importance of dietary intervention in controlling blood glucose levels (Table 3). Overall, the majority of the study participants (81.7%) had inadequate knowledge of diabetes, while only 18.3% demonstrated adequate knowledge of the condition as shown in Figure 1. Table 3. Knowledge on Diabetes among Study Participants. Variable Frequency (n=120) Percentage (%) Signs and Symptoms of Hyperglycaemia Extreme thirst 54 45.0 Frequent urination 64 53.3 Blurred vision 39 32.5 Tiredness/Fatigue 38 31.7 Weight lost 24 20.0 Signs and Symptoms of Hypoglycaemia Hunger 32 26.7 Nervousness/Jitteriness 33 27.5 Confusion 25 20.8 Mood swing irritability 23 19.2 Sweaty fast heart rate 19 15.8 How to Treat Hypoglycaemia Don’t know 79 65.8 Hard candy/Sugar/Sweet 15 12.5 Juice/Coke/Fanta 26 21.7 Frequency of Foot Checking None 91 71.1 Once a month 7 5.5 Once a week 9 7.0 Once a day 21 16.4 Importance of Foot Checking Don’t know 97 80.8 Prevent morbidity due to neuropathy 23 19.2 Frequency of Seeing an Eye Doctor When needed 103 85.8 At least once a year 17 14.2 Normal Range of Fasting Blood Glucose 4.0-5.9 mmol/L 18 15.0 6.0-10.00mmol/L 30 25.0 Don’t know 72 60.0 Normal Range of HbA1C 4.0-6.5% 5 4.2 7.0-8.0% 2 1.7 Don’t know 113 94.2 Long Term Complication of Diabetes Blindness 54 45.0 Kidney damage/dialysis 1 0.8 Amputation 32 26.7 Neuropathy/Impotence 0 0.0 Gastroparesis 0 0.0 Cardiovascular disease 49 40.8 Is Dietary Intervention Important in Controlling Blood Glucose Yes 1 0.8 No 119 99.2 Data presented as frequency and percentage.
HbA1C: glycated hemoglobin. Figure 1. Proportion of Knowledge Level on Diabetes among Study Participants. Sociodemographic and Clinical Factors Associated with Knowledge on Diabetes among Study Participants This study assessed sociodemographic and clinical factors associated with knowledge on diabetes among study participants. It was observed that gender (p=0.0150), family history of diabetes (p=0.0080), and specific family member with diabetes (p<0.0001) were significantly associated with diabetes knowledge level (Table 4). Ifthedurationofdiabetes(yearssincediagnosis)isnotstatisticallysignificanttoapatient’sknowledgeofthedisease,itimpliesthat experience with the disease does not automatically translate into improved knowledge. Ideally, a longer duration should lead to better disease management, but a lack of correlation suggests that passive experience is inferior to active, structured education Table 4. Sociodemographic and Clinical Factors Associated with Knowledge on Diabetes Among Study Participants.
Knowledge Level Variable Total (n=120) Adequate (n=22) Inadequate (n=98) Test Statistics p-value Age Group (Years) 0.018 0.9910 18-40 6 (5.0) 1 (4.5) 5 (5.1) 41-50 21 (17.5) 4 (18.2) 17 (17.3) ≥ 51 93 (77.5) 17 (77.3) 76 (77.6) Gender 5.976 0.0150 Male 18 (15.0) 7 (31.8) 11 (11.2) Female 102 (85.0) 15 (68.2) 87 (88.8) Ethnicity 0.135 0.9350 Akan 111 (92.5) 20 (90.9) 91 (92.9) Ewe 5 (4.2) 1 (4.5) 4 (4.1) Northerner 4 (3.3) 1 (4.5) 3 (3.1) Marital Status 2.861 0.4140 Single 10 (8.3) 1 (4.5) 9 (9.2) Divorced 20 (16.7) 2 (9.1) 18 (18.4) Widowed 37 (30.8) 6 (27.3) 31 (31.6) Married 53 (44.2) 13 (59.1) 40 (40.8) Educational Level 3.038 0.5520 No formal education 23 (19.2) 2 (9.1) 21 (21.4) Primary 18 (15.0) 4 (18.2) 14 (14.3) JHS/MSLC 67 (55.8) 14 (63.6) 53 (54.1) SHS 4 (3.3) 0 (0.0) 4 (4.1) Tertiary 8 (6.7) 2 (9.1) 6 (6.1) Religious Affiliation 4.511 0.1050 Christian 114 (95.0) 20 (90.9) 94 (95.9) Muslim 5 (4.2) 1 (4.5) 4 (4.1) Traditionalist 1 (0.8) 1 (4.5) 0 (0.0) Employment Status 0.118 0.9430 Unemployed 41 (34.2) 8 (36.4) 33 (33.7) Self-employed 72 (60.0) 13 (59.1) 59 (60.2) Employed 7 (5.8) 1 (4.5) 6 (6.1) Family History of Diabetes 7.124 0.0080 No 40 (33.3) 2 (9.1) 38 (38.8) Yes 80 (66.7) 20 (90.9) 60 (61.2) Specific Family Member (If Yes) 27.584 < 0.0001 Parent 28 (35.0) 1 (5.0) 27 (45.0) Siblings 22 (27.5) 5 (25.0) 17 (28.3) Grandparents 1 (1.3) 0 (0.0) 1 (1.7) Uncle 4 (5.0) 2 (10.0) 2 (3.3) Auntie 7 (8.8) 0 (0.0) 7 (11.7) Parent and Siblings 18 (22.5) 12 (60.0) 6 (10.0) Duration of Diabetes (Years) 4.876 0.0870 < 2 25 (20.8) 1 (4.5) 24 (24.5) 2-5 47 (39.2) 9 (40.9) 38 (38.8) ≥ 6 48 (40.0) 12 (54.5) 36 (36.7) Data presented as frequency (percentage).
P-values were computed by chi-square/Fischer exact test. P-values bolded and < 0.05 were considered statistical significance. Sociodemographic and Clinical Predictors of Knowledge on Diabetes Among Study Participants Table 5 depicts sociodemographic and clinical predictors of inadequate diabetes knowledge. In the univariate logistic regression model, female participants were 3.69 times more likely to have inadequate knowledge compared to their male counterparts [crude odds ratio (cOR) = 3.69, 95% confidence interval (CI) (2.17-39.62), p = 0.0030]. Also, participants who had a family history of diabetes had decreased odds of demonstrating inadequate knowledge of diabetes [cOR = 0.16, 95% CI (0.04- 0.71), p = 0.0170]. However, participants with parent [cOR = 54.99, 95% CI (5.84-498.96), p = 0.0080] and siblings [cOR = 6.80, 95% CI (1.68-27.52), p < 0.0001] as family members with diabetes had increased odds of inadequate diabetes knowledge as compared to those with both parents and siblings.
After adjusting for possible confounders in the multivariate logistic regression analysis, being female [aOR = 9.27, 95% CI = (2.17-39.62), p = 0.0030], having a family history of diabetes [aOR = 0.07, 95% CI = (0.01-0.43), p = 0.0040] and having a sibling with a history of diabetes [aOR = 8.66, 95% CI = (1.81-41.31), p = 0.0070] were identified as independent predictors of inadequate knowledge of diabetes (Table 5 ). Table 5. Sociodemographic and Clinical Predictors of Knowledge on Diabetes Among Study Participants. Variable Inadequate Knowledge (n=98) cOR (95% CI) p-value aOR (95% CI) p-value Age Group (Years) 18-40 5 (5.1) 1.00 - 1.00 - 41-50 17 (17.3) 0.85 (0.08-9.44) 0.8950 90638.28 (0.00-inf) 0.9980 ≥ 51 76 (77.6) 0.89 (0.10-8.16) 0.9210 2.99 (0.00-inf) 0.9970 Gender Male 11 (11.2) 1.00 - 1.00 - Female 87 (88.8) 3.69 (1.24-11.03) 0.0190 9.27 (2.17-39.62) 0.0030 Ethnicity Akan 91 (92.9) 1.52 (0.15-15.35) 0.7240 - - Ewe 4 (4.1) 1.33 (0.06-31.12) 0.8580 - - Northerner 3 (3.1) 1.00 - - - Marital Status Single 9 (9.2) 2.93 (0.34-25.33) 0.3300 - - Divorced 18 (18.4) 2.93 (0.60-14.33) 0.1860 - - Widowed 31 (31.6) 1.68 (0.57-4.92) 0.3450 - - Married 40 (40.8) 1.00 - - - Educational Level No formal education 21 (21.4) 3.50 (0.40-30.34) 0.2560 - - Primary 14 (14.3) 1.17 (0.17-8.19) 0.8770 - - JHS/MSLC 53 (54.1) 1.26 (0.23-6.94) 0.7890 - - SHS 4 (4.1) 53849.16 (0.00-inf) 0.9990 - - Tertiary 6 (6.1) 1.00 - - - Religious Affiliation Christian 94 (95.9) 1.00 - - - Muslim 4 (4.1) 0.85 (0.09-8.03) 0.8880 - - Traditionalist 0 (0.0) 0.00 (0.00-inf) > 0.999 - - Employment Status Unemployed 33 (33.7) 1.00 - - - Self-employed 59 (60.2) 1.10 (0.41-2.93) 0.8480 - - Employed 6 (6.1) 1.46 (0.15-13.85) 0.7450 - - Family History of Diabetes No 38 (38.8) 1.00 - 1.00 - Yes 60 (61.2) 0.16 (0.04-0.71) 0.0170 0.07 (0.01-0.43) 0.0040 Specific Family Member (If Yes) Parent 27 (45.0) 54.00 (5.84-498.96) 0.0080 1.78 (0.00-inf) 0.9970 Siblings 17 (28.3) 6.80 (1.68-27.52) < 0.0001 8.66 (1.81-41.31) 0.0070 Grandparents 1 (1.7) 323094.97 (0.00-inf) > 0.999 7.92 (0.00-inf) 0.9990 Uncle 2 (3.3) 2.00 (0.22-17.89) 0.5350 2.97 (0.22-40.57) 0.4150 Auntie 7 (11.7) 323094.97 (0.00-inf) > 0.999 1.58 (0.00-inf) 0.9980 Parent and Siblings 6 (10.0) 1.00 - 1.00 - Duration of Diabetes (Years) < 2 24 (24.5) 1.00 - - - 2-5.
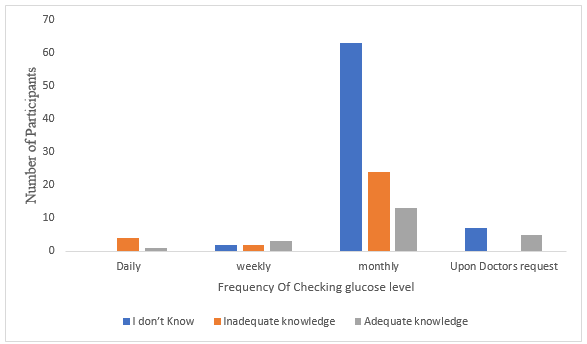
38 (38.8) 0.18 (0.02-1.48) 0.1100 - - ≥ 6 36 (36.7) 0.13 (0.02-1.03) 0.0530 - - P values were computed using univariate and multivariate logistic regression. p < 0.05 was considered statistically significant. Abbreviations: aOR, adjusted odds ratio; cOR, crude odds ratio; CI, confidence interval; inf, infinity. Participants’ knowledge on normal fasting blood glucose and frequency of laboratory checks The study accessed the participants knowledge on normal fasting blood glucose and frequency of glucose level checks. Over 65% of the participants did not know it is important to check their glucose level, whiles 20.5% had inadequate knowledge as shown in Figure 2. Figure 2. A graph showing the relationship between participants’ knowledge of normal fasting blood glucose and how often diabetics check their blood glucose level.
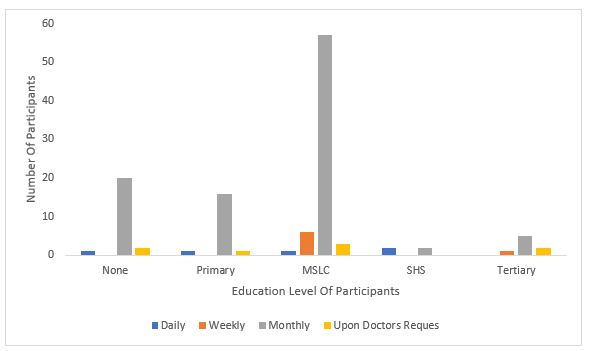
Education Level of diabetics and how often they check their glucose level The study accessed the educational level of diabetics and frequency of glucose checks. Chi Square analysis was done to determine the relationship between a person’s education level and practices. Most of the participants irrespective of their educational levels mostly checked their blood glucose level at the wrong time (monthly) as shown on figure 3. Figure 3. A graph showing the relationship between Education Level of diabetics and how often they check their glucose level.
Discussion
The sociodemographic information of the participants is presented in table 1, a total of 120 participants took part in the study. Overwhelming majority of the participants were females and this is in line with other research findings which had more female diabetic patients than males. This shows that females have a higher risk of developing diabetes than males (29,30,23). It is believed that male subjects generally live healthy lives as compared to their female counterparts who were more overweight (31). The finding is consistent with four studies conducted in Ghana, India, Pakistan and Ethiopia (32,33,34,31). As much as three-quarters of the respondents represented the 50+ age group, with less than one-fourth representing the ages group of 41-50.
These values are consistent with other studies which prove that the aged are more likely to be diagnosed with diabetes (29). Regarding the participants’ marital status, a majority were married. This has double edged implications. A study on diabetes knowledge and self-care practices where the majority of participants are married has significant implications for family-centred care, as spouses are the primary source of social support, diet regulation, and medication management. While marriage often provides a supportive environment, studies also show that being married can sometimes introduce barriers, such as complex household dynamics, or, conversely, act as a facilitator of better self-care, particularly when spousal support is high (35, 36) In term of educational status, more than two-thirds of the participants had moderate educational level of primary through JHS to SHS.
The primary implication of majority of participants having only a moderate education is that standardized diabetes education and practice are likely ineffective for this specific population. This creates a critical gap between clinical guidelines and the patients’ actual ability to implement self-care. This is consistent with the study outcome of (20) which reported that, diabetic patients with lower educational levels often possess poor knowledge, resulting in inadequate self-care practices, particularly regarding blood glucose monitoring and foot care. While medication adherence may be high, low literacy frequently hinders dietary management and long-term glyceamic control (37,20). The study found that, a little over half of the respondents had a history of diabetes in their families.
Majority with diabetic family members reported that it was their parents who had the disease. This claim is consistent with research conducted by (38) which suggested that diabetes could be a hereditary disease. Diabetes as a hereditary disease can be attributed to hereditary hemochromatosis (HH). The genetic disorder hereditary hemochromatosis (HH) results in an iron overload due to the uncontrolled absorption of iron from the intestines which is believed to primarily cause a defect in the early response of insulin to glucose (38). This study initially sought to assess diabetes knowledge among participants. The study observed that over twothirds of the participants had inadequate knowledge about diabetes. This prevalence is higher than that of a study conducted in Ghana which observed almost half of the participants had inadequate knowledge of diabete (39).
This high prevalence may be explained by the low educational and socioeconomic status of the current study population. It is worth noting that, there was a significant association between gender and knowledge of diabetes. Women had 9.27 odds of having inadequate knowledge compared to men. This finding is consistent with two previous studies conducted in Ghana that reported women being less likely to have adequate knowledge compared to men (39, 23). This study also revealed that participants with a family history of diabetes were 9.10 times less likely to have inadequate knowledge on diabetes. Individuals with a family history of diabetes are often exposed to discussions and medical consultations related to the condition within their households and thus have higher diabetes knowledge Further outcome reveals that half of the participants had adequate knowledge when asked about the signs and symptoms of high blood sugar, and one-third of the respondents had inadequate knowledge relating to the same subject matter.
In a study conducted in Pakistan to assess the knowledge of diabetic patients, it was found that knowledge about diabetic symptoms, risk factors, complications, and presentation substantially correlated with one’s degree of education (31). In our study most of the participants had at least a basic level of education and so it is quite appreciable as to why half of them had adequate knowledge about the symptoms. On the other hand, when asked about the symptoms of low blood sugar 50% of the population had no idea and the remaining 50% either had inadequate knowledge or adequate knowledge. Another interesting finding of this research was that a little over two-thirds of the participants had no idea on how to treat hypoglycaemia.
Astronomically, majority of the participants were ignorant of the fact that a diabetic must check his or her feet regularly and as high as 80.8 % of the participants did not know the importance of a diabetic patient regularly checking his feet. Most of the participants (more than half) had no knowledge about the normal fasting blood glucose level, a quarter had inadequate knowledge and only 15% of the participants knew the correct normal fasting blood glucose level. Regarding participants’ normal HbAIC almost all the participants had no idea about it. Only 6.7 % of participants were aware of the times a diabetic should exercise within a week. The remaining larger participants either had no knowledge or inadequate knowledge about how often a diabetic should exercise.
Lastly when asked about their knowledge on the long-term complications of uncontrolled diabetes the statistics are as follows that a little over one-third each of the participants had no knowledge, inadequate knowledge and adequate knowledge. Regarding Participants’ practices two-thirds of the participants ate on time while the remaining participants were not consistent with their eating times or frequently starved themselves.Skippingbreakfastislinkedtoobesityandahigher risk of type 2 diabetes. People with later chronotypes, who favour later bed and wake times, frequently skip breakfast. Research conducted to assess the validity of the above claim concluded that participants who usually skipped breakfast had significantly higher HbA1C levels, higher body mass indices (BMI) than those who are consistent with their breakfast eating time (40).
Also, regarding the intake of salt among diabetics, 85% showed a positive attitude by resisting the temptation of adding extra salt to already prepared food. Out of 120 participants only one gave a negative attitude answer when asked whether he smokes or not, all the participants (100%) were not in any way exposed to passive smoking. Also, a significant number representing 87.5% of the participants did not consume alcohol. Among the basic practices of a diabetic patient, as high as 83% and 89% never visited an eye clinic and never checked his or her feet respectively. Lastly, on the questions asked to assess the practices among diabetics, only 4.2% and 3.3 % daily checked their blood glucose level and blood pressure level respectively.
Approximately 83.3% checked their blood glucose levels monthly and 85% also checked their blood pressure monthly. In relating the educational level of participants to how often they check their glucose level, it was discovered that most of the participants usually checked their blood glucose levels on a monthly basis and it is attributed to the fact that most of them had their education level terminated at the pre tertiary level or had no education background at all. To further confirm that education has a significant impact on patients’ knowledge of their illness, the research of (22) in the northern part of Ghana showed a strong correlation between educational attainment and the participants’ degree of knowledge about diabetes.
Also, according to (22) participants with tertiary education demonstrated a much better level of knowledge than their less educated colleagues. This fact contrasted with our study as none of the 8 participants who had tertiary education checked their glucose levels regularly. A study in Khulna Diabetic Centre, Khulna, Bangladesh also showed a substantial difference between educational groups regarding understanding of the ideal blood glucose level for DM control (41). In their studies 122 out of the184 participants had little or no education and 62 were well educated. Out of the 122 with little or no education only 22 which represented 18% percent had an idea of the correct blood glucose level, also out of the 62 only 21 of them knew the correct blood glucose range (41).
The study assessed the relationship between knowledge of normal fasting blood glucose and how often diabetics check their blood glucose level. From the graph it clearly shows that most participants had no idea about what the normal fasting blood sugar is and with a p value of 0.008 it significantly impacted how often they check their blood sugar level. With a p value of less than 0.001, participants knowledge on how often they should visit the eye clinic affected how often they visited the hospital. A total of 84 participants had either inadequate knowledge or no knowledge on how often they should visit the eye clinic with 60 participants never having visited the eye clinic.
Also, with a p-value of 0.001 it clearly showed that the knowledge participants had on the normal HbAIC significantly impacted how often they check their blood pressure level. Knowledge of diabetes has been recognized as an important factor in adherence to the self-care practices of diabetes. The probability of a patient to be informed about a particular action or step in the management process of diabetes depends on the patient’s knowledge of the illness. Thus, those who are likely to comprehend their sickness and engage in self-management practices such as exercise, blood sugar testing, diet, regular foot examinations and many others are patients who have more knowledge about the illness (42).
It has been demonstrated that diabetic self-care behaviours are influenced by diabetes health literacy, which is a measure of knowledge (43). In consistency with the above results relating to the knowledge levels of a diabetic patient and their practices, a study conducted by (43) looked at the mediating role of diabetes knowledge in the relationship between diabetes health literacy and self-care practices. This study found that lower health literacy was significantly correlated with less diabetes knowledge, lower levels of physical activity, higher glycated haemoglobin (HbA1c) levels and less selfcontrol of glucose levels (43). In a study conducted at Korlebu Teaching Hospital in Accra, Ghana, it was discovered that out of the 390 diabetic patients who volunteered to undertake the research, only 26.4 percent knew the type of diabetes they had and only 3.8 percent of those with diabetes mellitus were aware that it could impact eye refraction; no patient mentioned that diabetes mellitus could result in cataract or diabetic retinopathy (44).
In considering years of experience with diabetes and knowledge, the study found no significant association. If the duration of diabetes (years since diagnosis) is not statistically significant to a patient’s knowledge of the disease, it implies that experience with the disease does not automatically translate into improved knowledge. Ideally, a longer duration should lead to better disease management, but a lack of correlation suggests that passive experience is inferior to active, structured education
Conclusion
Most of the participants demonstrated low knowledge level when they were assessed and this negatively impacted their attitude and self-care practices. The concludes that having a high knowledge about diabetes is a major step in the treatment and management process of diabetes and must be of a greater concern to both health care practitioners and the patients. Limitations Participants in our study were chosen from a hospital’s diabetic clinic, where they had the opportunity to learn a little bit about managing diabetes from the doctors and clinic staff. Therefore, their opinions might not be representative of all people with diabetes, including those who are undiagnosed and those who seek out non-biomedical treatments.
Recommendations We recommend that health care providers intensify education on self-care and management or selfcare practices to prevent diabetic complications. The level of awareness of diabetic complications among diabetic patients will increase with the organization of health education programs and health outreaches on preventive measures including adjusting to lifestyle and dietary alterations. Declarations Acknowledgements The authors would like to thank the study participants, hospital personnel, research assistants, and volunteers who all helped make the study a success. Authors’ contributions ROLES: Conceptualization. Data curation, formal analysis, methodology, writing-original draft Email: [email protected], AFFILIATION: Department of Hospitality and Tourism Education, University of Skill Training and Entrepreneurial Development. Kumasi-Ghana Data Availability All data generated or analyzed during this study are included in this article and raw data can be requested from the Competing Interests The authors declare no conflicts of interest.
Funding This study was funded by Kwame Nkrumah University of Science and Technology Research Fund (KRef), Kumasi- Ghana. Grant reference number-VC/OGR/15
Figures and Tables
| Variable Facility | Frequency (n=120) | Percentage (%) |
|---|---|---|
| Ejisu Government Hospital | 60 | 50.0 |
| Onwe Government Hospital Age Group (Years) | 60 | 50.0 |
| 18-40 | 6 | 5.0 |
| 41-50 | 21 | 17.5 |
| ≥ 51 Gender | 93 | 77.5 |
| Male | 18 | 15.0 |
| Female Ethnicity | 102 | 85.0 |
| Akan | 111 | 92.5 |
| Ewe | 5 | 4.2 |
| Northerner Marital Status | 4 | 3.3 |
| Single | 10 | 8.3 |
| Divorced | 20 | 16.7 |
| Widowed | 37 | 30.8 |
| Married Educational Level | 53 | 44.2 |
| No formal education | 23 | 19.2 |
|---|---|---|
| Primary | 18 | 15.0 |
| JHS/MSLC | 67 | 55.8 |
| SHS | 4 | 3.3 |
| Tertiary Religious Affiliation | 8 | 6.7 |
| Christian | 114 | 95.0 |
| Muslim | 5 | 4.2 |
| Traditionalist Employment Status | 1 | 0.7 |
| Unemployed | 41 | 34.2 |
| Self-employed | 72 | 60.0 |
| Employed | 7 | 5.8 |
| Variable Family History of Diabetes | Frequency (n=120) | Percentage (%) |
|---|---|---|
| No | 40 | 33.3 |
| Yes Specific Family Member (If Yes) | 80 | 66.7 |
| Parent | 28 | 35.0 |
| Siblings | 22 | 27.5 |
| Grandparents | 1 | 1.3 |
| Uncle | 4 | 5.0 |
| Auntie | 7 | 8.8 |
| Parent and Siblings Duration of Diabetes (Years) | 18 | 22.5 |
| < 2 | 25 | 20.8 |
| 2-5 | 47 | 39.2 |
| ≥ 6 Diabete Drugs | 48 | 40.0 |
| Metformin | 83 | 69.2 |
| Glibernclamide | 3 | 2.5 |
| Metformin and glibenclamide | 33 | 27.5 |
| Insulin Do you have any other NCDs | 1 | 0.8 |
| No | 28 | 23.3 |
| Yes Specific Other NCD (If Yes) | 92 | 76.7 |
| Hypertension | 92 | 100.0 |
| Variable Signs and Symptoms of Hyperglycaemia | Frequency (n=120) | Percentage (%) |
|---|---|---|
| Extreme thirst | 54 | 45.0 |
| Frequent urination | 64 | 53.3 |
| Blurred vision | 39 | 32.5 |
| Tiredness/Fatigue | 38 | 31.7 |
| Weight lost Signs and Symptoms of Hypoglycaemia | 24 | 20.0 |
| Hunger | 32 | 26.7 |
| Nervousness/Jitteriness | 33 | 27.5 |
| Confusion | 25 | 20.8 |
| Mood swing irritability | 23 | 19.2 |
| Sweaty fast heart rate How to Treat Hypoglycaemia | 19 | 15.8 |
| Don’t know | 79 | 65.8 |
| Hard candy/Sugar/Sweet | 15 | 12.5 |
| Juice/Coke/Fanta Frequency of Foot Checking | 26 | 21.7 |
| None | 91 | 71.1 |
| Once a month | 7 | 5.5 |
| Once a week | 9 | 7.0 |
| Once a day Importance of Foot Checking | 21 | 16.4 |
| Don’t know | 97 | 80.8 |
| Prevent morbidity due to neuropathy Frequency of Seeing an Eye Doctor | 23 | 19.2 |
| When needed | 103 | 85.8 |
| At least once a year Normal Range of Fasting Blood Glucose | 17 | 14.2 |
| 4.0-5.9 mmol/L | 18 | 15.0 |
| 6.0-10.00mmol/L | 30 | 25.0 |
| Don’t know Normal Range of HbA1C | 72 | 60.0 |
| 4.0-6.5% | 5 | 4.2 |
| 7.0-8.0% | 2 | 1.7 |
|---|---|---|
| Don’t know Long Term Complication of Diabetes | 113 | 94.2 |
| Blindness | 54 | 45.0 |
| Kidney damage/dialysis | 1 | 0.8 |
| Amputation | 32 | 26.7 |
| Neuropathy/Impotence | 0 | 0.0 |
| Gastroparesis | 0 | 0.0 |
| Cardiovascular disease Is Dietary Intervention Important in Controlling Blood Glucose | 49 | 40.8 |
| Yes | 1 | 0.8 |
| No | 119 | 99.2 |
| Knowledge Level | |||||
|---|---|---|---|---|---|
| Variable | Total (n=120) | Adequate (n=22) | Inadequate (n=98) | Test Statistics | p-value |
| Age Group (Years) | 0.018 | 0.9910 | |||
| 18-40 | 6 (5.0) | 1 (4.5) | 5 (5.1) | ||
| 41-50 | 21 (17.5) | 4 (18.2) | 17 (17.3) | ||
| ≥ 51 | 93 (77.5) | 17 (77.3) | 76 (77.6) | ||
| Gender | 5.976 | 0.0150 | |||
| Male | 18 (15.0) | 7 (31.8) | 11 (11.2) | ||
| Female | 102 (85.0) | 15 (68.2) | 87 (88.8) | ||
| Ethnicity | 0.135 | 0.9350 |
| Akan | 111 (92.5) | 20 (90.9) | 91 (92.9) | ||
|---|---|---|---|---|---|
| Ewe | 5 (4.2) | 1 (4.5) | 4 (4.1) | ||
| Northerner | 4 (3.3) | 1 (4.5) | 3 (3.1) | ||
| Marital Status | 2.861 | 0.4140 | |||
| Single | 10 (8.3) | 1 (4.5) | 9 (9.2) | ||
| Divorced | 20 (16.7) | 2 (9.1) | 18 (18.4) | ||
| Widowed | 37 (30.8) | 6 (27.3) | 31 (31.6) | ||
| Married | 53 (44.2) | 13 (59.1) | 40 (40.8) | ||
| Educational Level | 3.038 | 0.5520 | |||
| No formal education | 23 (19.2) | 2 (9.1) | 21 (21.4) | ||
| Primary | 18 (15.0) | 4 (18.2) | 14 (14.3) | ||
| JHS/MSLC | 67 (55.8) | 14 (63.6) | 53 (54.1) | ||
| SHS | 4 (3.3) | 0 (0.0) | 4 (4.1) | ||
| Tertiary | 8 (6.7) | 2 (9.1) | 6 (6.1) | ||
| Religious Affiliation | 4.511 | 0.1050 | |||
| Christian | 114 (95.0) | 20 (90.9) | 94 (95.9) | ||
| Muslim | 5 (4.2) | 1 (4.5) | 4 (4.1) | ||
| Traditionalist | 1 (0.8) | 1 (4.5) | 0 (0.0) | ||
| Employment Status | 0.118 | 0.9430 | |||
| Unemployed | 41 (34.2) | 8 (36.4) | 33 (33.7) | ||
| Self-employed | 72 (60.0) | 13 (59.1) | 59 (60.2) | ||
| Employed | 7 (5.8) | 1 (4.5) | 6 (6.1) | ||
| Family History of Diabetes | 7.124 | 0.0080 | |||
| No | 40 (33.3) | 2 (9.1) | 38 (38.8) | ||
| Yes | 80 (66.7) | 20 (90.9) | 60 (61.2) | ||
| Specific Family Member (If Yes) | 27.584 | < 0.0001 | |||
| Parent | 28 (35.0) | 1 (5.0) | 27 (45.0) | ||
| Siblings | 22 (27.5) | 5 (25.0) | 17 (28.3) | ||
| Grandparents | 1 (1.3) | 0 (0.0) | 1 (1.7) | ||
| Uncle | 4 (5.0) | 2 (10.0) | 2 (3.3) | ||
| Auntie | 7 (8.8) | 0 (0.0) | 7 (11.7) | ||
| Parent and Siblings | 18 (22.5) | 12 (60.0) | 6 (10.0) | ||
| Duration of Diabetes (Years) | 4.876 | 0.0870 | |||
| < 2 | 25 (20.8) | 1 (4.5) | 24 (24.5) | ||
| 2-5 | 47 (39.2) | 9 (40.9) | 38 (38.8) | ||
| ≥ 6 | 48 (40.0) | 12 (54.5) | 36 (36.7) |
| Variable Age Group (Years) | Inadequate Knowledge (n=98) | cOR (95% CI) | p-value | aOR (95% CI) | p-value |
|---|---|---|---|---|---|
| 18-40 | 5 (5.1) | 1.00 | - | 1.00 | - |
| 41-50 | 17 (17.3) | 0.85 (0.08-9.44) | 0.8950 | 90638.28 (0.00-inf) | 0.9980 |
| ≥ 51 Gender | 76 (77.6) | 0.89 (0.10-8.16) | 0.9210 | 2.99 (0.00-inf) | 0.9970 |
| Male | 11 (11.2) | 1.00 | - | 1.00 | - |
| Female Ethnicity | 87 (88.8) | 3.69 (1.24-11.03) | 0.0190 | 9.27 (2.17-39.62) | 0.0030 |
| Akan | 91 (92.9) | 1.52 (0.15-15.35) | 0.7240 | - | - |
| Ewe | 4 (4.1) | 1.33 (0.06-31.12) | 0.8580 | - | - |
| Northerner Marital Status | 3 (3.1) | 1.00 | - | - | - |
| Single | 9 (9.2) | 2.93 (0.34-25.33) | 0.3300 | - | - |
| Divorced | 18 (18.4) | 2.93 (0.60-14.33) | 0.1860 | - | - |
| Widowed | 31 (31.6) | 1.68 (0.57-4.92) | 0.3450 | - | - |
| Married Educational Level | 40 (40.8) | 1.00 | - | - | - |
| No formal education | 21 (21.4) | 3.50 (0.40-30.34) | 0.2560 | - | - |
| Primary | 14 (14.3) | 1.17 (0.17-8.19) | 0.8770 | - | - |
| JHS/MSLC | 53 (54.1) | 1.26 (0.23-6.94) | 0.7890 | - | - |
| SHS | 4 (4.1) | 53849.16 (0.00-inf) | 0.9990 | - | - |
| Tertiary Religious Affiliation | 6 (6.1) | 1.00 | - | - | - |
| Christian | 94 (95.9) | 1.00 | - | - | - |
| Muslim | 4 (4.1) | 0.85 (0.09-8.03) | 0.8880 | - | - |
| Traditionalist Employment Status | 0 (0.0) | 0.00 (0.00-inf) | > 0.999 | - | - |
| Unemployed | 33 (33.7) | 1.00 | - | - | - |
| Self-employed | 59 (60.2) | 1.10 (0.41-2.93) | 0.8480 | - | - |
| Employed Family History of Diabetes | 6 (6.1) | 1.46 (0.15-13.85) | 0.7450 | - | - |
| No | 38 (38.8) | 1.00 | - | 1.00 | - |
| Yes Specific Family Member (If Yes) | 60 (61.2) | 0.16 (0.04-0.71) | 0.0170 | 0.07 (0.01-0.43) | 0.0040 |
| Parent | 27 (45.0) | 54.00 (5.84-498.96) | 0.0080 | 1.78 (0.00-inf) | 0.9970 |
| Siblings | 17 (28.3) | 6.80 (1.68-27.52) | < 0.0001 | 8.66 (1.81-41.31) | 0.0070 |
| Grandparents | 1 (1.7) | 323094.97 (0.00-inf) | > 0.999 | 7.92 (0.00-inf) | 0.9990 |
| Uncle | 2 (3.3) | 2.00 (0.22-17.89) | 0.5350 | 2.97 (0.22-40.57) | 0.4150 |
| Auntie | 7 (11.7) | 323094.97 (0.00-inf) | > 0.999 | 1.58 (0.00-inf) | 0.9980 |
| Parent and Siblings Duration of Diabetes (Years) | 6 (10.0) | 1.00 | - | 1.00 | - |
| < 2 | 24 (24.5) | 1.00 | - | - | - |
| 2-5. | 38 (38.8) | 0.18 (0.02-1.48) | 0.1100 | - | - |
| ≥ 6 | 36 (36.7) | 0.13 (0.02-1.03) | 0.0530 | - | - |
References
- Doherty, M. L., Owusu-Dabo, E., Kantanka, O. S., Brawer, R. O., & Plumb, J. D. (2014). Type 2 diabetes in a rapidly urbanizing region of Ghana, West Africa: A qualitative study of dietary preferences, knowledge and practices. BMC Public Health, 14(1). https://doi.org/10.1186/1471- 2458-14-1069
- Cho NH, Shaw JE, Karuranga S, Huang Y, da Rocha Fernandes JD, Ohlrogge AW, Malanda B. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res Clin Pract. 2018 Apr;138:271-281. doi: 10.1016/j.diabres.2018.02.023 Epub 2018 Feb 26. PMID: 29496507.
- Bekele, B. B. (n.d.). The prevalence of macro and microvascular complications of DM among patients in Ethiopia 1990-2017: Systematic review. Diabetes & Metabolic Syndrome, 13(1), 672–677. https://doi org/10.1016/j.dsx.2018.11.046
- Godman, B., Basu, D., Pillay, Y., Mwita, J. C., Mutashambara Rwegerera, G., Anand Paramadhas, B. D., Tiroyakgosi, C., Mbah Okwen, P., Campbell, S., Meyer, J. C., Sumner, A. E., Adam Mahmoud, M., Muniyappa, R., & Paramadhas, A. B. (2020). Review of Ongoing Activities and Challenges to Improve the Care of Patients With Type 2 Diabetes Across Africa and the Implications for the Future. Frontiers in Pharmacology | Www, 17, 108. https://doi.org/10.3389/fphar.2020.00108
- Kazibwe J, Gad M, Abassah-Konadu E, Amankwah I, Owusu R, Gulbi G, et al. (2024) The epidemiological and economic burden of diabetes in Ghana: A scoping review to inform health technology assessment. PLOS Glob Public Health 4(3): e0001904.
- Gojka Roglic. (2016). WHO Global report on diabetes: A summary. 1, 3–8.Groop, L., & Pociot, F. (2014). Genetics of diabetes - Are we missing the genes or the disease? Molecular and Cellular Endocrinology, 382(1), 726–739. https://doi.org/10.1016/J.MCE.2013.04.002 7 Ong, K. L., Stafford, L. K., McLaughlin, S. A., Boyko, E. J., Vollset, S. E., Smith, A. E., ... & Brauer, M. (2023). Global, regional, and national burden of diabetes from 1990 to 2021, with projections of prevalence to 2050: a systematic analysis for the Global Burden of Disease Study 2021. The Lancet, 402(10397), 203-234.
- Hossain, M. J., Al-Mamun, M., & Islam, M. R. (2024). Diabetes mellitus, the fastest growing global public health concern: Early detection should be focused. Health science reports, 7(3), e2004. https://doi org/10.1002/hsr2.2004
- Fottrell E, Ahmed N, Shaha SK, Jennings H, Kuddus A, Morrison J, et al. (2018). Diabetes knowledge and care practices among adults in rural Bangladesh: a crosssectional survey. BMJ Global Health. 2018;3:e000891. https://doi.org/10.1136/bmjgh-2018-000891
- Young Choi, J., Ali, M. K., & Choi, D. (2024). Determinants of health and mortality in undiagnosed diabetes: A nationally representative US adult, 2011-2020. Diabetes research and clinical practice, 210, 111634. https://doi org/10.1016/j.diabres.2024.111634
- Velázquez López, L., Muñoz Torres, A. V., Medina Bravo, P. G., & Escobedo de la Peña, J. (2023). Inadequate diabetes knowledge is associated with poor glycemia control in patients with type 2 diabetes. Atencion primaria, 55(5), 102604. https://doi.org/10.1016/j aprim.2023.102604
- Wondie, Y., Minwuyelet, A., Bogale, A. D., Hailu, G., & Mengstie, E. A. (2025). Risk factors of diabetic ketoacidosis among patients with diabetes attending at public hospitals of East Gojjam Zone, Northwest Ethiopia: an unmatched case - control study. BMC endocrine disorders, 25(1), 222. https://doi.org/10.1186/ s12902-025-02023-x
- Sakyi, S. A., Opoku, S., Senu, E., Korsah, E. E., Effah, A., Baidoo, B. T., Arele, E. A., Frimpong, E., Naturinda, E., Kodzo, K. E., Amenuvor, A., Kwayie, A. A., Bannor, L. O., Ampofo, R. O., Marfo, B. A., & Mensah-Bonsu, R. O. (2023). Factors associated with knowledge and hypoglycemia experience among patients with diabetes mellitus in Ghana: A cross-sectional study. Public health challenges, 2(4), e130. https://doi.org/10.1002/puh2.130
- Wamucii,E.G.,Kyallo,F.,&Kiage,B.(2020).Knowledgeand self-care practices among diabetic patients-a case study ofThikalevel5hospital,Kenya.JHealthMedNurs,5,25-43.
- Borba, A. K. de O. T., Arruda, I. K. G., Marques, A. P. de O., Leal, M. C. C., & Diniz, A. da S. (2019). Knowledge and attitude about diabetes self-care of older adults in primary health care. Ciencia e Saude Coletiva, 24(1), 125–136. https://doi.org/10.1590/1413- 81232018241.35052016
- Gul, N. (2010). Knowledge, attitudes and practices of type 2 diabetic patients. Journal of Ayub Medical College Abbottabad, 22(3), 128-131.
- Moraes, N. M., Souza, G. F. P., Brito, F. I., Antonio, J. M. E., Cipriano, A. E (2020) Knowledge and self-care in diabetes mellitus and their correlations with sociodemographic, clinical and treatment variables. Diabetes Updates 6:
- Almomani, M. H., & Al-Tawalbeh, S. (2022). Glycemic Control and Its Relationship with Diabetes Self-Care Behaviors Among Patients with Type 2 Diabetes in Northern Jordan: A Cross-Sectional Study. Patient preference and adherence, 16, 449–465. https://doi org/10.2147/PPA.S343214
- Opoku, R., Ackon, S.K., Kumah, E. et al. (2023). Self-care behaviors and associated factors among individuals with type 2 diabetes in Ghana: a systematic review. BMC Endocr Disord 23, 256. https://doi.org/10.1186/s12902- 023-01508-x
- Tetteh C, Saah FI, Amu H. (2024). Diabetes selfmanagement: a qualitative study of education needs, practices and caregiver support in the Keta Municipality of Ghana. BMJ Public Health. 2:e000640. https://doi org/10.1136/bmjph-2023-000640
- Johnson, B. B., Jarvis, M. A., & Chipps, J. A. (2025). Selfmanagement knowledge, attitudes and practices among persons with type 2 diabetes in Ghana. African journal of primary health care & family medicine, 17(1), e1–e10. https://doi.org/10.4102/phcfm.v17i1.4696
- Adongo, R., Id, A., Bam, V., Azongo, T. B., & Afaya Id, A. (2020). Knowledge of chronic complications of diabetes among persons living with type 2 diabetes mellitus in northern Ghana. https://doi.org/10.1371/journal pone.0241424
- Obirikorang,Y.,Obirikorang,C.,Anto,E.O.,Acheampong, E., Batu, E. N., Stella, A. D., Constance, O., & Brenya, P. K. (2016). Knowledge of complications of diabetes mellitus among patients visiting the diabetes clinic at Sampa Government Hospital, Ghana: A descriptive study. BMC Public Health, 16(1). https://doi.org/10.1186/s12889- 016-3311-7
- Rothman, R. L., Malone, R., Bryant, B., Wolfe, C., Padgett, P., DeWalt, D. A., Weinberger, M., & Pignone, M. (2005). The spoken knowledge in low literacy in diabetes scale: A diabetes knowledge scale for vulnerable patients. Diabetes Educator, 31(2), 215–224. https://doi org/10.1177/0145721705275002
- Ahmed, I. bin, Binnwejim, M. S., Alnahas, T. M., Asaad, A., Raes, A., Basamad, M. A., Alqurashi, A. E., Alotaibi, L. T., Alqasem, R. M., Ghazwani, S. M., Almuyidi, S. M., Alshehri, W. A., Alfuhigi, Z. D., Nasser, M., & Almeshref, H. (2019). Level of diabetic patients’ knowledge of diabetes mellitus, its complications and management.
- Al-Maskari, F., El-Sadig, M., Al-Kaabi, J. M., Afandi, B., Nagelkerke, N., & Yeatts, K. B. (2013a). Knowledge, Attitude and Practices of Diabetic Patients in the United Arab Emirates. PLoS ONE, 8(1). https://doi.org/10.1371/ journal.pone.0052857
- Noordzij, M., et al., (2010). Sample size calculations: basic principles and common pitfalls. Nephrology dialysis transplantation. 25(5): p. 1388-1393
- Subish P, Leelavathy DA. Knowledge, attitude, and practice outcomes: Evaluating the impact of counseling in hospitalized diabetic patients in India. P T J. 2006;31:389–92.
- Gautam, A., Bhatta, D. N., & Aryal, R. U. (2015). Diabetes related health knowledge, attitude and practice among diabetic patients in Nepal. BMC Endocrine Disorders, 15(1). https://doi.org/10.1186/s12902-015-0021-6
- Mekonnen, C. K., Abate, H. K., & Tegegne, E. T. (2020). Knowledge, attitude, and practice toward lifestyle modification among diabetes mellitus patients attending the university of gondar comprehensive specialized hospital Northwest, Ethiopia. Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy, 13, 1969–1977. https://doi.org/10.2147/DMSO.S250787
- Nisar, N., Khan, I. A., Qadri, M. H., & Sher, S. A. (2008). Knowledge and risk assessment of diabetes mellitus at primary care level: a preventive approach required combating the disease in a developing country. Pak J Med Sci, 24(5), 667-72.
- Valckx, S. D. M., De Pauw, I., De Neubourg, D., Inion, I., Berth, M., Fransen, E., ... & Leroy, J. L. M. R. (2012). BMIrelated metabolic composition of the follicular fluid of women undergoing assisted reproductive treatment and the consequences for oocyte and embryo quality. Human reproduction, 27(12), 3531-3539.
- Gulabani, M., John, M., & Isaac, R. (2008a). Knowledge of diabetes, its treatment and complications amongst diabetic patients in a tertiary care hospital. Indian Journal of Community Medicine : Official Publication of Indian Association of Preventive & Social Medicine, 33(3), 204–206. https://doi.org/10.4103/0970-0218.42068
- Kawaguchi, T., Takahashi, H., & Gerber, L. H. (2023). Clinics in liver disease: update on nonalcoholic steatohepatitis: sarcopenia and nonalcoholic fatty liver disease. Clinics in Liver Disease, 27(2), 275-286.
- Pratiwi, I. N., Nursalam, N., Widyawati, I. Y., & Ramoo, V. (2024). Spousal Involvement in Collaborative Management and Glycemic Behavior Change among Patients with Diabetes Mellitus: A Systematic Review. SAGE open nursing, 10, 23779608241245196. https:// doi.org/10.1177/23779608241245196
- Mphasha, M. H., Mothiba, T. M., & Skaal, L. (2022). Family support in the management of diabetes patients’ perspectives from Limpopo province in South Africa. BMC public health, 22(1), 2421. https://doi.org/10.1186/ s12889-022-14903-1
- Yimer M., Nezif, H. (2021). Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy:14 535–54
- Utzschneider, K. M., & Kowdley, K. V. (2010). Hereditary hemochromatosis and diabetes mellitus: implications for clinical practice. Nature Reviews Endocrinology, 6(1), 26-33.
- Afaya, R.A., et al., (2020). Knowledge of chronic complications of diabetes among persons living with type 2 diabetes mellitus in northern Ghana. Plos one. 15(10): p. e0241424.
- Reutrakul, S., Hood, M. M., Crowley, S. J., Morgan, M. K., Teodori, M., & Knutson, K. L. (2014). The relationship between breakfast skipping, chronotype, and glycemic control in type 2 diabetes. Chronobiology international, 31(1), 64-71.
- Hoque, M. A., Islam, M. S., Khan, M. A. M., & Ahasan, H. N. (2009). Knowledge of diabetic complications in a diabetic population. Journal of Medicine, 10(2), 90-93.
- Kugbey, N., Oppong Asante, K., & Adulai, K. (2017). Illness perception, diabetes knowledge and self-care practices among type-2 diabetes patients: a cross-sectional study. BMC research notes, 10(1), 381.
- Van Der Heide, I., Uiters, E., Rademakers, J., Struijs, J. N., Schuit, A. J., & Baan, C. A. (2014). Associations among health literacy, diabetes knowledge, and selfmanagement behavior in adults with diabetes: results of a dutch cross-sectional study. Journal of health communication, 19(sup2), 115-131.
- Ovenseri Ogbomo, G. O. (2013). Knowledge of diabetes and its associated ocular manifestations by diabetic patients: A study at Korle Bu Teaching Hospital, Ghana. Nigerian Medical Journal, 54(4).
This is a text version generated from the article. For the formatted version of record (with original tables & figures), download the PDF →