Full Text Hide / show
Background
: Blood culture remains the gold standard for diagnosing bloodstream infections and guiding antimicrobial therapy; however, contamination during sample collection continues to compromise diagnostic accuracy and patient management. This prospective observational study was conducted over six months in the Department of Microbiology of a tertiary care teaching hospital to evaluate the burden and impact of false-positive blood cultures. Results: A total of 670 blood culture samples were processed using the automated BACT/ALERT system, followed by organism identification and antimicrobial susceptibility testing using standard microbiological methods and the VITEK 2 system. Among the processed samples, 44 (6.6%) were identified as contaminants. Micrococcus species and Coagulase-negative Staphylococci were the predominant isolates, each accounting for 40.9% of contaminants, followed by Gram-positive bacilli.
Contamination was most frequently observed in emergency and critical care settings. False-positive blood cultures contributed to diagnostic uncertainty, repeated sampling, delayed confirmation of true pathogens, unnecessary empirical antibiotic exposure, increased laboratory workload, prolonged hospitalization, and additional healthcare costs. The study highlights the importance of strict aseptic blood collection practices, continuous staff training, diagnostic stewardship, and regular surveillance to reduce contamination rates and improve overall quality patient care. Keywords: Contaminants,Improper Blood Collection,False Positive Blood Culture,High Risk Areas,Diagnostic Stewardship.
Introduction
Blood culture remains the cornerstone for diagnosing bloodstream infections and sepsis, playing a critical role in pathogen identification and guiding targeted antimicrobial therapy. The reliability of blood culture results is largely dependent on pre-analytical factors, including appropriate timing of collection, adequate blood volume, and strict adherence to aseptic techniques. Proper skin antisepsis, use of sterile equipment, and preference for peripheral venipuncture are essential to minimize errors. Despite advancements in automated diagnostic systems, including platforms such as the VITEK 2 system, pre-analytical errors continue to significantly impact the accuracy and clinical utility of blood cultures Contaminated blood cultures constitute a substantial proportion of positive results and remain a major source of diagnostic uncertainty.
Foundational work by Keri K. Hall and Jason A. Lyman (1), along with subsequent studies (2–9), has established improper collection techniques as the primary contributor.Morerecentevidencehighlightsthatthischallenge persists despite technological progress. A large retrospective study demonstrated that contamination rates can still range around 3–4% even in modern healthcare settings (10), while multicenter analyses emphasize significant variability in definitions, surveillance, and reporting practices across institutions (11). Emerging data from low- and middle-income settings further highlight the need for diagnostic stewardship, showing persistent contamination trends over time and the impact of healthcare system factors on culture quality (12). Quality improvement initiatives have demonstrated that targeted interventions, including staff training and standardized protocols, can reduce contamination rates but require sustained implementation (13).
Additionally, recent ecological analyses during healthcare resource constraints reinforce the importance of optimizing blood culture utilization and minimizing unnecessary sampling (14). False-positive results due to contamination frequently lead to unnecessary or prolonged antimicrobial therapy, repeated blood culture sampling, additional investigations, and increased healthcare costs. These practices contribute significantly to antimicrobial resistance and patient morbidity, highlighting a critical gap between diagnostic capability and sample integrity. AIM & OBJECTIVES 1. To determine the prevalence of false-positive blood cultures in a tertiary care teaching hospital. 2. To identify the common contaminating organisms associated with blood culture collection. 3. To evaluate high-risk hospital areas associated with increased contamination rates. 4. To assess the impact of blood culture contamination on patient management, laboratory workload, and healthcare costs.
5. To emphasize the importance of strict aseptic blood collection practices and diagnostic stewardship in reducing contamination rates and improving quality patient care.
Materials and Methods
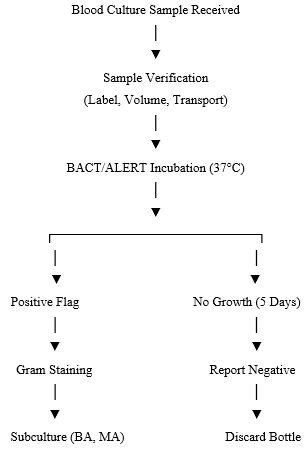
This prospective observational study was conducted in the Department of Microbiology of a tertiary care teaching hospital over a period of six months. All blood culture samples received during the study period were included, irrespective of patient age. Samples from immunocompromised individuals, including infants, neonates, pregnant women, patients on chemotherapy, and HIV-positive patients, were excluded. Blood culture bottles incubated beyond five days were also excluded from analysis.Blood samples were collected under aseptic precautions and inoculated into aerobic blood culture bottles, which were transported promptly to the laboratory. All samples were processed using the automated blood culture system (BACT/ALERT) and incubated at 37°C. Bottles flagged positive were subjected to Gram staining, followed by subculture onto Blood agar and McConkey agar.
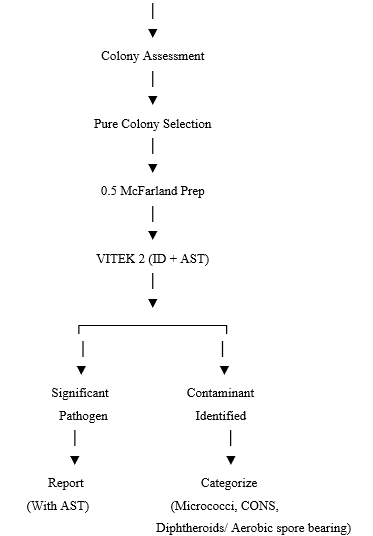
Plates were incubated aerobically at 37°C and examined for growth. Isolates were identified based on standard microbiological techniques, including colony morphology, Gram staining, and biochemicalreactions,withconfirmationbyautomatedsystems where applicable. Antimicrobial susceptibility testing was performed using the VITEK 2 system and interpreted according to Clinical and Laboratory Standards Institute (CLSI) guidelines. Blood cultures yielding organisms commonly considered skin commensals, such as Coagulase-negative Staphylococci (CoNS), Diphtheroids, and Micrococcus, were classified as contaminants in the absence of supportive clinical evidence. Relevant demographic and clinical data, including the source of the sample (ward/unit), were recorded and analyzed. Blood culture bottles showing no growth after five days of incubation were reported as negative and discarded as per laboratory protocol.
Data were analyzed using descriptive statistics, and contamination rates were expressed as percentages. Figure 1. Workflow of Blood Culture Processing and Identification of Contaminants. Blood culture samples were processed using the BACT/ALERT system. Positive bottles underwent Gram staining, subculture, and identification using the VITEK 2 system. Isolates were categorized as clinically significant pathogens or contaminants based on microbiological findings and clinical correlation. Negative bottles after 5 days were discarded.
Results
A total of 670 blood culture samples were processed during the study period. Of these, 44 samples (6.6%) were identified as contaminants.The study population included equal numbers of males and females. The mean age was approximately 56 years, with a higher proportion of contaminated samples observed among elderly patients above 60 years. Microbiological analysis showed that Micrococcus species and Coagulase-negative Staphylococci were the predominant contaminants, each accounting for 40.9% of isolates. Gram-positive bacilli accounted for 18.2%. Table 1. Various contaminants in the total samples received. Organism Category Frequency (n) Percentage (%) Micrococcus 18 40.9% CONS (various species) 18 40.9% GPB (including diphtheroids) 8 18.2% Total = 44 100% Contamination was predominantly observed in emergency outpatient settings followed by intensive care units and hemodialysis unit.
| Ward/ Area Of Collection | Micrococcus | Cons | GPB | Other | Total |
|---|---|---|---|---|---|
| CHEST & TB WARD | 0 | 2 | 0 | 0 | 2 |
| Emergency Dept OP | 6 | 7 | 3 | 1 | 17 |
| Casualty –ER | 3 | 1 | 1 | 0 | 5 |
| Emergency Dept - IP | 1 | 0 | 0 | 0 | 1 |
| MICU (all) | 2 | 5 | 3 | 0 | 10 |
| HDU (all) | 6 | 0 | 0 | 0 | 6 |
| GM WARD | 0 | 2 | 0 | 0 | 2 |
| Casualty- OP | 0 | 0 | 1 | 0 | 1 |
| TOTAL | 19 | 18 | 8 | 1 | 44 |
Discussion
Blood culture contamination remains a persistent and clinically significant problem in routine microbiology practice, directly affecting diagnostic accuracy, antimicrobial stewardship, healthcare expenditure, and overall quality patient care. Although acceptable contamination rates are generally recommended to remain below 3%, the present study demonstrated a contamination rate of 6.6%, indicating a substantial burden within the studied healthcare setting (1,5,16). This finding raises concern that contamination burden may be considerably higher in healthcare settings with larger patient loads, including government hospitals and high-volume centralized laboratories, where increased workload and limited resources may further compromise adherence to optimal aseptic blood collection practices and proper handling of culture bottles during transport to the laboratory.
The predominant contaminants isolated were Micrococci and Coagulase-Negative Staphylococci, each accounting for 40.9% of isolates, followed by Gram-positive bacilli. These organisms, being part of normal skin flora, are frequently introduced during blood collection because of inadequate skin antisepsis, improper handling, or breaches in aseptic precautions during venipuncture (7,8,15). Their isolation often creates a major diagnostic dilemma, particularly in critically ill patients where differentiating contamination from true bloodstream infection becomes challenging. A significant observation in the present study was the higher frequency of contamination in emergency outpatient settings, MICU, and HDU. Similar findings have been reported in previous studies involving emergency departments and intensive care settings (3,4,22). High patient turnover, urgent clinical interventions, repeated venous access, staff workload, and time-sensitive decision-making in these areas may compromise adherence to standard aseptic blood collection practices.
Such high-acuity environments therefore remain particularly vulnerable to blood culture contamination. False-positive blood culture reports have important implications for quality patient care. Contaminated cultures frequently result in unnecessary empirical antibiotic administration, repeated blood sampling, delayed confirmation of true pathogens, prolonged hospital stay, and additional diagnostic investigations. In critically ill patients, delays in obtaining accurate microbiological results may postpone definitive antimicrobial therapy and adversely affect clinical outcomes. Furthermore, inappropriate antimicrobial exposure resulting from false-positive reports may contribute to antimicrobial resistance and increased treatment-related complications (8,14,23). Beyond patient management, contamination significantly increases laboratory workload and healthcare costs. Repeat culture processing, additional organism identification, susceptibility testing, prolonged reporting time, and repeated investigations consume considerable laboratory resources and healthcare expenditure (12,13,17,21,23).
In resourcelimited healthcare settings, these avoidable burdens may further strain already limited infrastructure and negatively impact delivery of timely healthcare services. The findings of the present study emphasize that blood culture contamination should not be viewed merely as a laboratory error, but rather as an important healthcare quality and patient safety issue involving clinicians, nursing staff, microbiologists, infection control teams, and hospital administration. Prevention of blood culture contamination primarily depends on meticulous aseptic precautions during sample collection, proper skin antisepsis, standardized blood collection protocols, and regular training of healthcare personnel involved in phlebotomy practices (9–11,14,18,19,24). Since contamination was predominantly observed in emergency and critical care settings, targeted interventions in these high-risk areas may provide greater benefit than generalized hospital-wide measures.
Limitations
This study has certain limitations. Being a single-center observational study with predominantly descriptive analysis, the findings may not be generalizableto all healthcare settings. Additionally, exact economic burden and patient outcome measures such as duration of hospitalization and mortality were not quantified. However, this study highlights important real-world implications of blood culture contamination in routine clinical practice.
Conclusion
Blood culture contamination remains a major yet preventable challenge in healthcare, significantly affecting diagnostic accuracy, antimicrobial stewardship, patient outcomes, laboratory efficiency, and healthcare expenditure. Delayed or misleading blood culture reports may result in inappropriate antimicrobial therapy, prolonged hospitalization, increased healthcare burden, and avoidable morbidity, particularly in critically ill patients and resource-limited settings. Reducing contamination requires strict adherence to aseptic blood collection practices, continuous training of healthcare personnel, standardized collection protocols, and regular surveillance of contamination rates. Strengthening diagnostic stewardship and implementing continuous quality improvement measures are essential to improve the reliability of blood culture reporting, optimize antimicrobial use, reduce unnecessary healthcare costs, and enhance overall quality patient care. Future efforts should focus on multicentric evaluations, continuous quality monitoring, and adoption of improved diagnostic strategies to enhance reliability and strengthen quality of care, particularly in resource-limited settings.
Figures and Tables
| Organism Category | Frequency (n) | Percentage (%) |
|---|---|---|
| Micrococcus | 18 | 40.9% |
| CONS (various species) | 18 | 40.9% |
| GPB (including diphtheroids) | 8 | 18.2% |
| Total = | 44 | 100% |
References
- Hall KK, Lyman JA. Updated review of blood culture contamination. Clin Microbiol Rev. 2006;19(4):788–802.
- Min H, Park CS, Kim DS, Kim KH. Blood culture contamination in hospitalized patients. Korean J Pediatr. 2014;57(4):178–185.
- Aiesh BM, et al. Blood culture contamination in a tertiary care hospital. BMC Infect Dis. 2023;23:448.
- Hemeg HA, Almutairi AZ, et al. Patterns and risk factors of blood culture contamination. Saudi Med J. 2020;41(5):508–515.
- Bekeris LG, Tworek JA, Walsh MK, Valenstein PN. Trends in blood culture contamination rates. Arch Pathol Lab Med. 2005;129(10):1222–1225.
- Snyder SR, Favoretto AM, Baetz RA, et al. Effectiveness of interventions to reduce blood culture contamination. Am J Clin Pathol. 2012;138(6):827–832.
- Self WH, Speroff T, Grijalva CG, et al. Reducing blood culture contamination in the emergency department. Infect Control Hosp Epidemiol. 2013;34(6):582–587.
- Alahmadi YM, Aldeyab MA, McElnay JC, et al. Clinical and economic impact of contaminated blood cultures. J Hosp Infect. 2011;77(3):233–236.
- Doern GV, Carroll KC, Diekema DJ, et al. Practical guidance for clinical microbiology laboratories. Clin Infect Dis. 2020;71(6):e109–e116.
- Multiyear blood culture contamination study. BMC Infect Dis. 2025.
- Standardized surveillance of blood culture contamination. J Clin Microbiol. 2025.
- Saleh L, et al. Diagnostic stewardship and blood culture utilization. Antimicrob Steward Healthc Epidemiol. 2025.
- Patel P, et al. Quality improvement initiatives to reduce contamination. BMJ Open Qual. 2025.
- Salomão MC, et al. Stewardship interventions in blood culture contamination. Open Forum Infect Dis. 2026.
- Aiesh BM, Daraghmeh D, Abu-Shamleh N, et al. Blood culture contamination in a tertiary care hospital: a retrospective three-year study. BMC Infect Dis. 2023;23:448.
- Alhumaid S, et al. Multiyear experience with blood culture contamination rates in a tertiary care hospital. BMC Infect Dis. 2025;25:11908.
- Szymczak EG, et al. Blood culture contamination: analysis and associated laboratory costs. Int J Environ Res Public Health. 2022;19(5):3009.
- Saleh L, Chamieh A, El Basst R, et al. Trends in blood culture contamination and diagnostic stewardship. Antimicrob Steward Healthc Epidemiol. 2025;5(1):e27.
- Sautter RL, Parrott JS, Nachamkin I, et al. Evidencebased practices to reduce blood culture contamination. Clin Microbiol Rev. 2024;37(4):e00087-24.
- Koroki T, Fujii M, Kotani Y, et al. Arterial versus venous blood culture contamination in critically ill patients. Clin Infect Dis. 2026;82(3):446–452.
- Dempsey C, Skoglund E, Muldrew KL, Garey KW. Economic burden of blood culture contamination. Am J Infect Control. 2019;47(8):963–967.
- Martínez JA, et al. Blood culture contamination in emergency departments: risk factors and outcomes. J Hosp Infect. 2020;105(3):469–475.
- Gander RM, et al. Impact of blood culture contamination on antibiotic use and outcomes. Infect Control Hosp Epidemiol. 2019;40(9):1013–1019.
- Salomão MC, et al. Reduction of blood culture contamination through stewardship interventions. Open Forum Infect Dis. 2026;13(Suppl 1):ofaf695.
This is a text version generated from the article. For the formatted version of record (with original tables & figures), download the PDF →