Full Text Hide / show
Introduction
Urinary tract infections (UTIs) represent one of the most common bacterial infections globally and pose a major public health challenge due to their high prevalence, associated morbidity, and economic impact. These infections can affect various components of the urinary system, including the urethra, bladder, and kidneys, and are associated with clinical manifestations such as dysuria, increased urinary frequency, flank pain, and fever. Without appropriate treatment, UTIs may progress to severe complications, including renal damage, systemic infections, and recurrent episodes [1-3, 4-5]. From an etiological standpoint, UTIs are primarily caused by bacteria, most commonly enterobacteria originating from the intestinal microbiota. Among these, Escherichia coli is the predominant pathogen, followed by Klebsiella pneumoniae, Proteus mirabilis, Enterococcus faecalis, and Staphylococcus saprophyticus.
However, the distribution of uropathogens varies depending on patient demographics, clinical context, and geographic region [1-2, 4-6, 7]. The increasing prevalence of antimicrobial resistance among uropathogens has become a major concern worldwide. This phenomenon is largely driven by empirical antibiotic use and misuse, particularly when microbiological data are unavailable. The emergence of multidrug-resistant organisms, especially extended-spectrum β-lactamase (ESBL)-producing strains, significantly complicates treatment and increases the risk of poor clinical outcomes [1-4, 7-8]. Moreover, regional differences in microbial ecology and resistance patterns emphasize the importance of local epidemiological surveillance to guide appropriate empirical therapy [3-4, 9]. In developing countries, including Morocco, this challenge is further compounded by factors such as selfmedication, unregulated antibiotic access, and variability in prescribing practices.
Despite these concerns, data remain limited in certain regions, including Béni Mellal. The present study aims to characterize the bacterial profile of UTIs and analyze antimicrobial susceptibility patterns in the Béni Mellal region. We hypothesize that Escherichia coli is the predominant pathogen, alongside a diverse microbial spectrum, with high levels of antimicrobial resistance, including multidrug-resistant phenotypes. The findings are expected to contribute to improved empirical treatment strategies and support rational antibiotic use at the local level.
Patients and Methods
Patients This was an analytical study conducted on 800 urine samples collected from both outpatients and hospitalized patients who underwent a urine cytobacteriological examination (ECBU). Demographic data, including patients’ age and sex, were retrieved from the laboratory information system. The study was carried out in the bacteriology laboratory of the Regional Hospital Center of Beni Mellal and encompassed all ECBU tests performed during the study period. The primary objective was to assess the prevalence of bacterial urinary tract infections and to determine the antibiotic susceptibility profiles of the isolated pathogens. The study population included all patients who underwent an ECBU during this period. Only samples demonstrating significant bacterial growth were included in the analysis.
Polymicrobial samples, considered to be contaminated, as well as incomplete records, were excluded. Methods Sample Collection and Bacterial Isolation Urine samples were collected aseptically, primarily using the midstream clean-catch method, in accordance with standard recommendations. Specimens were promptly transported to the laboratory and processed without delay to ensure result reliability. Cytobacteriological examination included macroscopic and microscopic analyses (leukocytes, erythrocytes, and bacteria), as well as bacterial culture. Samples were inoculated onto appropriate media: CLED (Cystine Lactose Electrolyte Deficient), a non-selective medium supporting the growth of both Gram-positive and Gram-negative bacteria, and EMB (Eosin Methylene Blue), a selective and differential medium for Gram-negative bacteria. Cultures were incubated at 37 °C for 18 to 24 hours, in accordance with ECAST (2017) recommendations.
Bacterial Identification
Samples with bacterial counts ≥10⁵ CFU/mL were considered positive. Isolated colonies were characterized based on morphology and Gram staining: Gram-positive bacteria appeared purple, whereas Gram-negative bacteria appeared pink. Identification of non-fastidious Gram-negative bacilli was performed using the API 20E system, which consists of 20 microtubes containing dehydrated substrates for assessing carbohydrate fermentation and enzymatic activities such as β-galactosidase and urease. The microtubes were inoculated with a bacterial suspension, incubated at 37 °C for 24 hours, and interpreted using the manufacturer’s reference table or the APIWEB software. Differentiation between Streptococcus and Staphylococcus species was achieved using the catalase test: bubble formation upon contact with 3% hydrogen peroxide indicates Staphylococcus.
Pathogenic Staphylococcus strains (S. aureus) were further confirmed by positive DNase and coagulase tests. Antimicrobial Susceptibility Testing The antimicrobial susceptibility of bacterial isolates was assessed using the disk diffusion method on Mueller-Hinton agar, in accordance with current EUCAST/CLSI guidelines. Antibiotic-impregnated disks at standardized concentrations were applied to the agar surface using a dispenser, allowed to diffuse for 3 minutes at room temperature, and then incubated at 37 °C for 24 hours. The antibiotics tested covered several classes, including amoxicillin, ticarcillin, amoxicillin/clavulanic acid (Augmentin), ciprofloxacin, trimethoprim-sulfamethoxazole (Bactrim), mecillinam, piperacillin/tazobactam, cefotaxime, and cefoxitin. Inhibition zones were interpreted according to ECAST (2017) guidelines to classify isolates as susceptible (S), intermediate (I), or resistant (R).
Statistical Analysis
Data analysis was performed using SPSS and Excel software. Qualitative variables were expressed as frequencies and percentages. The chi square test (χ²) was used to assess the association between the type of isolated bacterium and the variables age, sex, and patient status (Ambulatory vs hospitalized). The threshold for statistical significance was set at p < 0.05.
Results
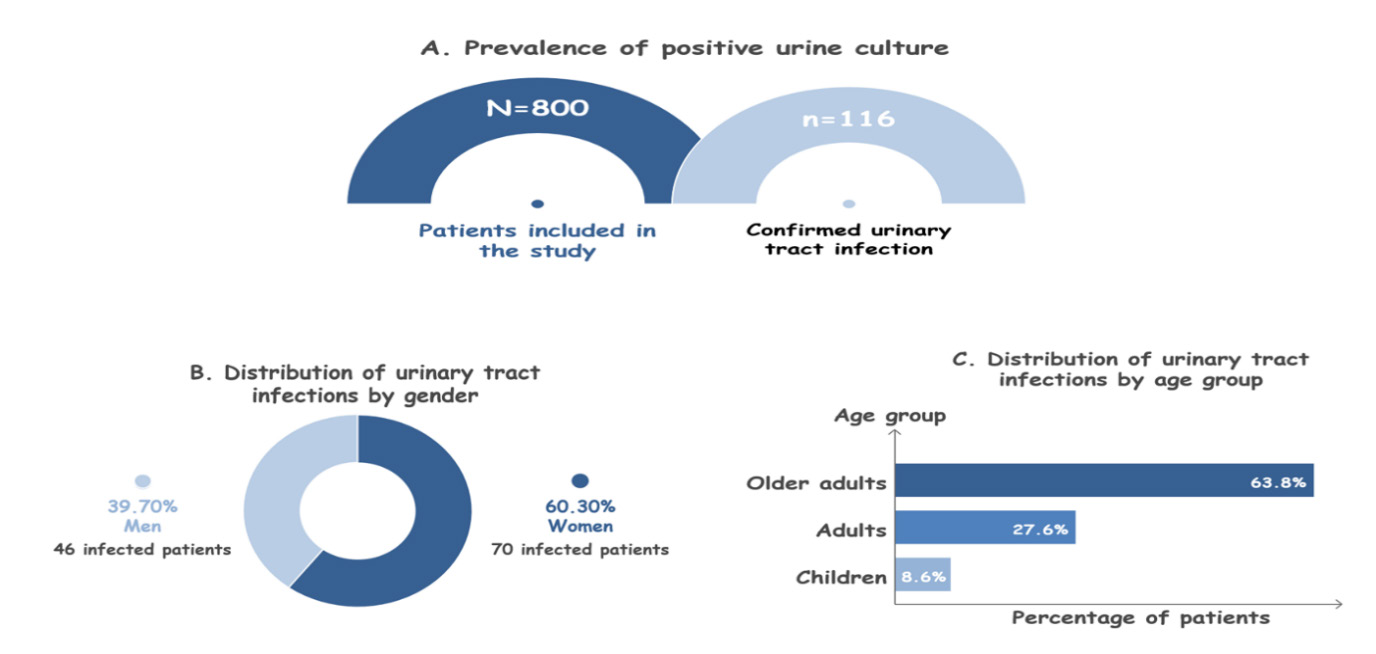
Demographic Characteristics of Patients Among the 800 patients included in this study, 116 cases of urinary tract infection confirmed by a positive urine cytobacteriological examination (ECBU) were identified, corresponding to a prevalence of 14.5% (Figure 1, A). A female predominance was observed among these cases, with 70 women (60.3%) compared to 46 men (39.7%) (Figure 1, B). Analysis of the age distribution revealed a marked predominance of elderly patients, who accounted for 63.8% of cases (n = 74), followed by adults (27.6%, n = 32) and children (8.6%, n = 10) (Figure 1, C). These findings highlight a higher frequency of urinary tract infections among the elderly, as well as a female predominance within this population.
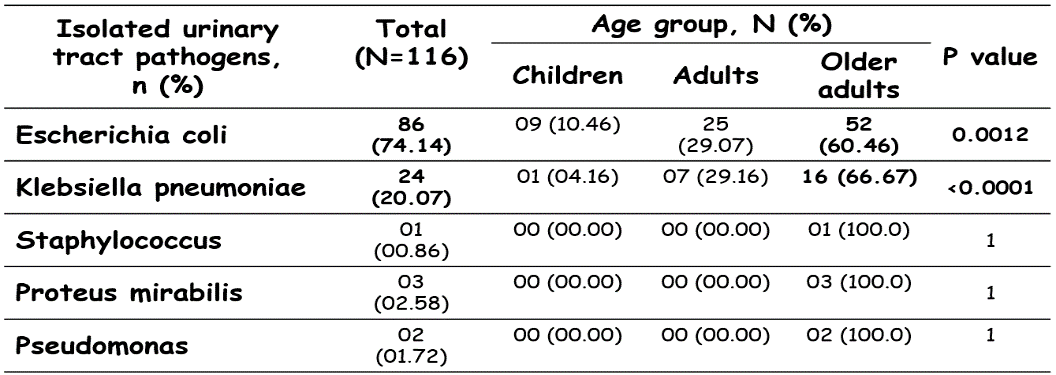
Figure 1. Demographic Characteristics of Patients. Analysis of the distribution of isolated uropathogens by age group among the included patients The analysis of the distribution of uropathogens isolated from 116 patients with positive urine cultures, stratified by age groups, revealed a clear predominance of Escherichia coli (74.14%), followed by Klebsiella pneumoniae (20.07%). Furthermore, a significant overrepresentation of these two bacterial species was observed among elderly patients (Escherichia coli: 60.46%, p = 0.0012; Klebsiella pneumoniae: 66.7%, p < 0.0001) (Table 1). These findings highlight the critical role of advanced age as a major risk factor for the occurrence of urinary tract infections, particularly those involving opportunistic and potentially multidrug-resistant pathogens.In addition, these results suggest an increased susceptibility of older populations to atypical uropathogens compared to the enterobacteria classically implicated.
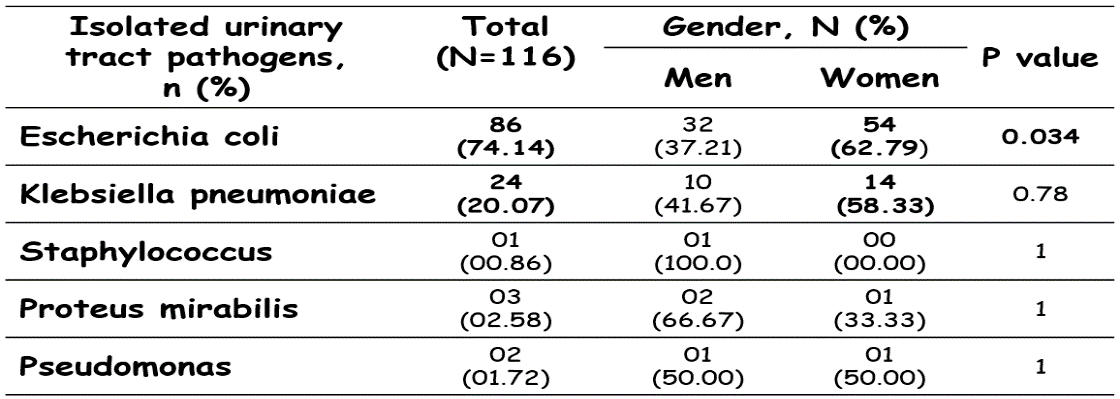
This heightened vulnerability may be explained by mechanisms such as immunosenescence, as well as the high prevalence of comorbidities in this age group. Table 1. The distribution of isolated uropathogens by age group. Analysis of the distribution of isolated urinary pathogens by sex of the included patients The gender-stratified analysis of uropathogen distribution among the 116 included patients revealed that Escherichia coli was the most prevalent isolate (74.14%), followed by Klebsiella pneumoniae (20.07%). Notably, E. coli was significantly more common in women than in men respectively (62.79% vs 37.21%, p = 0.034), while no significant gender differences were observed for Klebsiella pneumoniae (58.33 % vs 41.67%, p = 0.78) or the less frequent isolates, including Staphylococcus (0.86%), Proteus mirabilis (2.58%), and Pseudomonas (1.72%) (Table 2).
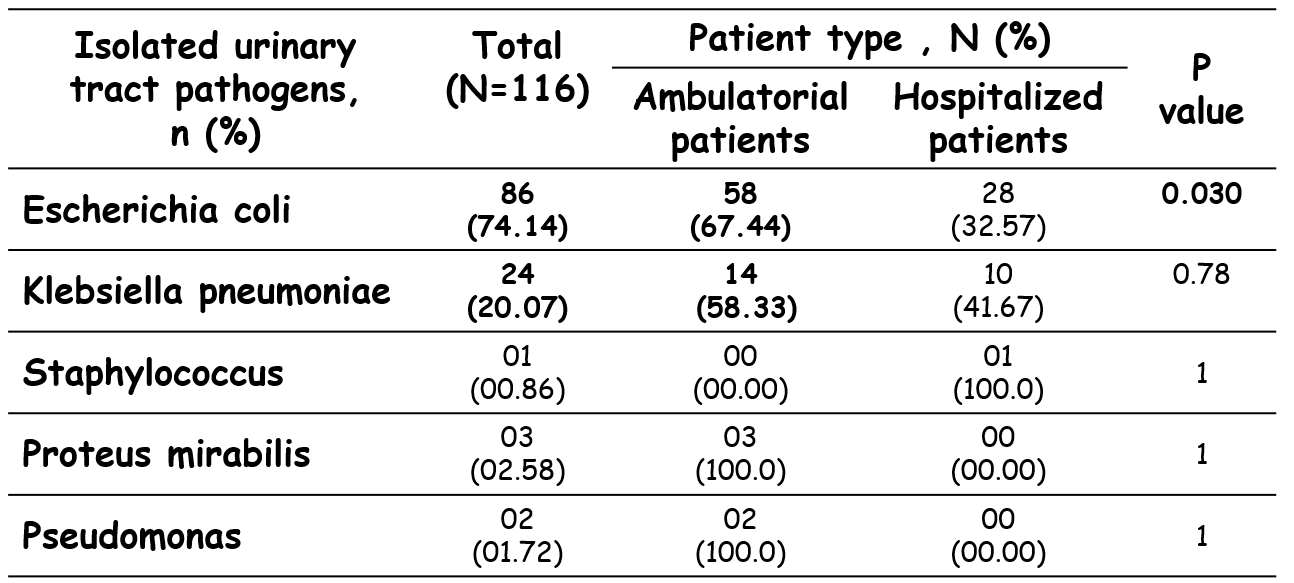
These findings underscore the female predominance of E. coli in urinary tract infections, consistent with anatomical and physiological predispositions, whereas other uropathogens did not demonstrate a statistically significant gender bias. Table 2. The distribution of isolated urinary pathogens by sex. Analysis of the distribution of isolated uropathogens by patient type (ambulatory vs hospitalized) among the included patients The distribution of uropathogens isolated from outpatients and hospitalized patients is presented in Table 3. A significantly higher proportion of Escherichia coli isolates was observed among outpatients (67.44%; n = 58) compared to hospitalized patients (32.57%; n = 28) (p = 0.030). In contrast, Klebsiella pneumoniae was more frequently isolated from outpatients (58.33%; n = 14) than from hospitalized patients (41.67%; n = 10); however, this difference was not statistically significant (p = 0.78) (Table 3).
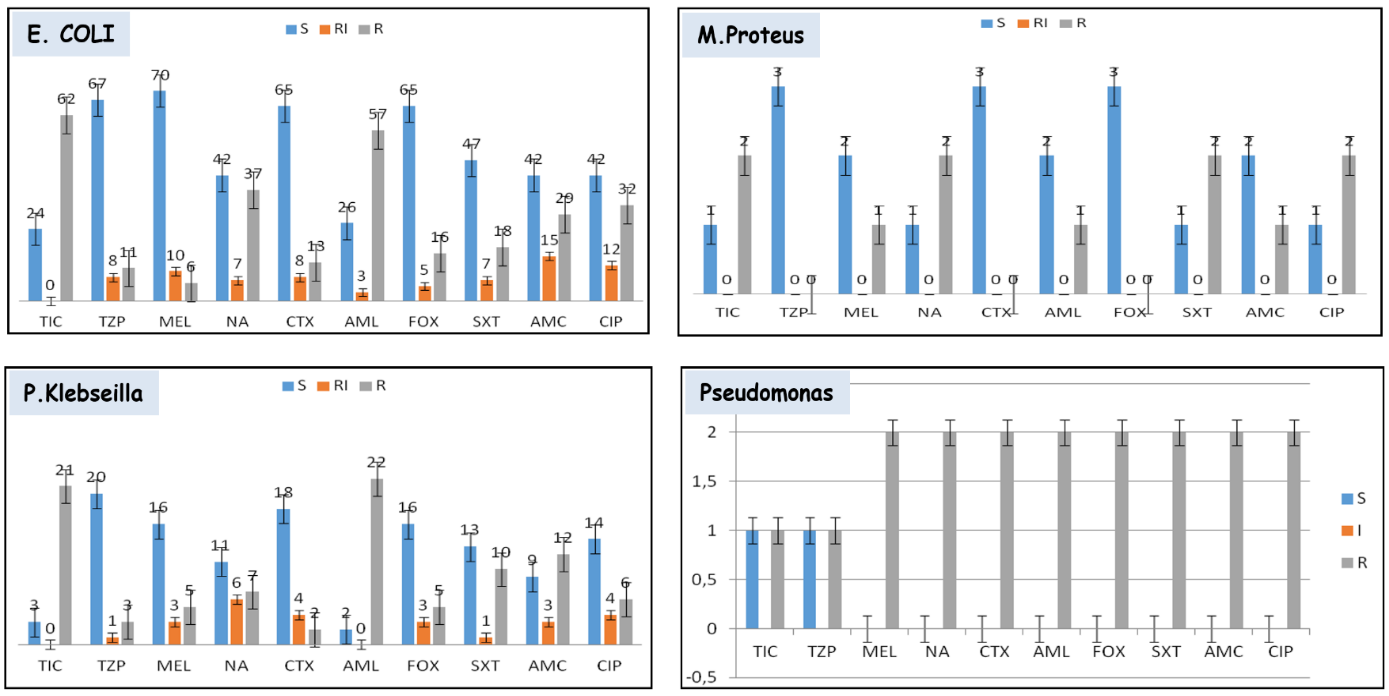
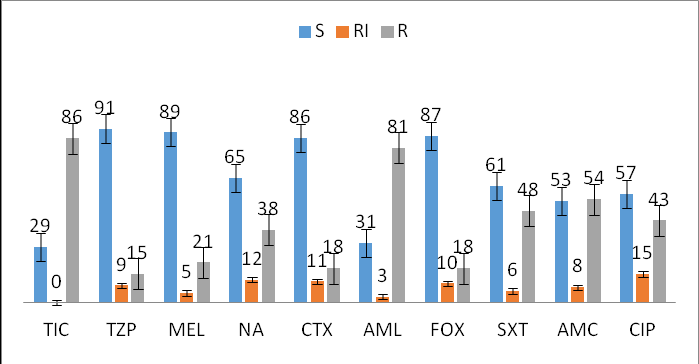
Table 3. The distribution of isolated uropathogens by patient type (ambulatory vs hospitalized). Profile of antibiotic resistance of urinary pathogens isolated in this study The overall analysis of antibiotic susceptibility profiles, illustrated in Figure 2, highlights a concerning prevalence of antibiotic resistance among the main uropathogens isolated. High resistance is observed against unprotected penicillins, particularly amoxicillin and ticarcillin, as well as against some commonly prescribed agents such as ciprofloxacin and trimethoprim– sulfamethoxazole. In contrast, the best antibacterial activities are associated with mecillinam, the piperacillin–tazobactam combination, and third generation and related cephalosporins (cefotaxime, cefoxitin) (Figure 2). Figure 2. Profiles of sensitivity and resistance to antibiotics. Abbreviation: TIC: Ticarcillin, AMC: Amoxicillin–clavulanic acid, NA: Nalidixic acid, TZP: Piperacillin–tazobactam, CTX: Cefotaxim, FOX: Cefoxitin , SXT: Trimethoprim–sulfamethoxazole, CIP: Ciprofloxacin, AML: Amoxicillin, MEL: Mecillinam, S:Susceptible, RI: intermediate resistance, R: resistance.
In Escherichia coli, the predominant pathogen, quantitative data confirm a high level of resistance to ticarcillin (72 %), amoxicillin (66 %), and nalidixic acid (43 %), as shown by the distribution of phenotypes in Figure 3. Intermediate resistance is also observed for amoxicillin–clavulanic acid and trimethoprim–sulfamethoxazole. In contrast, high susceptibility is maintained for mecillinam (82 %) and piperacillin–tazobactam (80 %), as well as for cephalosporins (cefotaxime and cefoxitin, 75 %), suggesting their therapeutic relevance in this setting (Figure 3). The profile of Klebsiella spp. appears similar but with increased variability, marked by notable resistance to classical beta lactams and relatively preserved efficacy of cephalosporins and mecillinam. This heterogeneity may reflect the diversity of resistance mechanisms, including the production of extended spectrum beta lactamases (Figure 3).
For Proteus mirabilis, the results indicate full susceptibility to piperacillin–tazobactam–based combinations and to cephalosporins (cefotaxime, cefoxitin), while substantial resistance is observed for ticarcillin, nalidixic acid, ciprofloxacin, and trimethoprim–sulfamethoxazole. However, interpretation of these results should be cautious due to the limited sample size, as suggested by the narrow spread of values in Figure 3. Finally, Pseudomonas species stand out by a marked multidrug resistant profile, with almost no susceptibility to most tested antibiotics, except for a marginal response to a few agents. This phenotype, clearly illustrated in Figure 3 by the predominance of bars corresponding to resistance, highlights the major therapeutic challenge posed by this opportunistic pathogen. Overall, these findings underscore a concerning evolution of bacterial resistance in urinary tract infections, justifying the need for tailored therapeutic strategies based on local susceptibility data and the reinforcement of policies promoting the appropriate use of antibiotics.
Discussion
Urinary tract infections (UTIs) remain a major public health concern due to their high incidence, potential morbidity, and the alarming rise in antimicrobial resistance. In our series of 800 urine cytobacteriological examinations (UCBE), the prevalence of confirmed infections was 14.5%. This rate falls within the range reported in Morocco and North Africa, where prevalence typically varies between 15% and 17% depending on study populations and recruitment criteria [10]. Beyond this consistency, our study provides updated data in a context where recent local information on microbiological profiles and resistance patterns remains limited, thereby enhancing its epidemiological relevance. From an etiological perspective, our findings confirm the clear predominanceofEscherichiacoli(74.14%),followedbyKlebsiella pneumoniae (20.07%), while other pathogens remain marginal (Table 1).
This distribution is consistent with international data identifying E. coli as the leading uropathogen and Klebsiella as the second most frequent agent [11]. However, the relatively high proportion of Klebsiella observed in our series, particularly in certain subgroups, may reflect a gradual shift toward more complex microbiological profiles, potentially driven by healthcare exposure and antibiotic use [12]. Age-stratified analysis revealed a higher concentration of cases among elderly patients, with an overrepresentation of E. coli and Klebsiella pneumoniae (Table 2). This finding aligns with the recognized role of aging as a major risk factor, associated with immunosenescence, multimorbidity, and functional urinary disorders [12]. It may also reflect contextual factors specific to our setting, including increased antibiotic exposure and more frequent healthcare utilization, which can promote the selection of opportunistic enterobacteria.
Sex distribution confirmed the predominance of E. coli infections among women, consistent with known anatomical and physiological mechanisms and supported by the literature [13]. The absence of significant sex-related differences for other pathogens suggests that sex-related determinants mainly influence uncomplicated communityacquired infections. Analysis according to patient status showed a predominance of E. coli in outpatient settings, indicating a substantial contribution of community-acquired infections in our cohort (Table 3). This trend is consistent with findings from other African and Moroccan studies reporting a predominance of community-associated enterobacteria in positive urine cultures [10]. It may also be influenced by local prescribing practices and relatively uncontrolled access to antibiotics, contributing to selective pressure in the community.
The antimicrobial resistance profile represents the most concerning aspect of our findings. The high resistance rates of E. coli to amoxicillin, ticarcillin, and nalidixic acid, along with notable resistance to ciprofloxacin and cotrimoxazole (Figure 3), reflect a loss of efficacy of antibiotics historically used as first-line treatments [11, 14]. This situation may be partly explained by the extensive and sometimes inappropriate use of these agents, including self-medication and empirical treatment without microbiological confirmation, a phenomenon widely described in middle-income countries. In contrast, certain antibiotics such as mecillinam, piperacillin- tazobactam, and some cephalosporins retain satisfactory activity (Figure 3). However, this observation should be interpreted with caution in a context marked by the increasing spread of extended-spectrum beta-lactamases (ESBLs) [11- 12, 15].
Klebsiella pneumoniae, in particular, is frequently associated with higher resistance levels, especially in hospital settings or in ESBL-producing strains, which is consistent with the heterogeneity observed in our series [12, 15]. The lack of molecularcharacterizationinourstudyrepresentsasignificant limitationinaccuratelyassessingtheseresistancemechanisms. The profiles of Proteus mirabilis and Pseudomonas spp. further illustrate the growing complexity of UTIs (Figure 3). While Proteus retains relative susceptibility to certain antibiotic classes, significant resistance to commonly used oral agents is already evident. Pseudomonas, on the other hand, exhibits a frequently multidrug-resistant profile, posing a major therapeutic challenge, particularly in vulnerable or hospitalized patients [12]. Nevertheless, several limitations must be acknowledged. The retrospective and monocentric design may limit the generalizability of our findings.
The lack of detailed clinical data prevents precise identification of associated risk factors and limits stratification according to infection severity or complexity. Furthermore, the absence of molecular analyses restricts the exploration of resistance mechanisms, particularly the true prevalence and dissemination dynamics of ESBL-producing strains. In clinical practice, these findings have direct implications for the management of UTIs in our setting. They highlight the need to adapt empirical antibiotic therapy to local resistance patterns [11, 16]. The empirical use of antibiotics such as amoxicillin, ciprofloxacin, or cotrimoxazole appears increasingly inappropriate without prior microbiological documentation. Conversely, antibiotics that retain satisfactory activity could be prioritized in updated local guidelines. These results also emphasize the importance of strengthening antimicrobial stewardship strategies and continuous microbiological surveillance to curb the progression of antimicrobial resistance [16].
Conclusion
This study confirms that urinary tract infections in the Beni Mellal region are predominantly caused by Escherichia coli, followed by Klebsiella pneumoniae, with a clear predominance among women and elderly patients. More concerningly, antimicrobial susceptibility patterns reveal a marked decline in the effectiveness of several agents commonly used in empirical therapy, including amoxicillin, ticarcillin, ciprofloxacin, and trimethoprim-sulfamethoxazole. In contrast, mecillinam, piperacillin-tazobactam, and certain cephalosporins have retained comparatively better in vitro activity, suggesting that they may represent more appropriate therapeutic options in this context, pending microbiological confirmation. Overall,thesefindingshighlighttheurgentneedforcontinuous local surveillance of uropathogens and their resistance profiles, as well as the implementation of antimicrobial stewardship strategies to promote rational prescribing and limit the spread of multidrug-resistant organisms.
Such measures are essential to improve the quality of care for patients with urinary tract infections and to preserve the effectiveness of available antimicrobial agents. Acknowledgements Conflict of Interest We declare that there are no conflicts of interest to disclose. Authors Contribution The authors of this article have made significant contributions to the design, data collection, analysis, and manuscript writing. Their individual contributions are as follows: Dr. Aazzane Oussama: Writing - original version, Conceptualization, Methodology, Data collection, Formal analysis, Visualization. Pr. Souad Mojahidi, Dr. Mohamed Belcaid, Dr.Hasnaa Bazhar, Mr. Youssef Hakiki, Mr. Khalid Abdelmoua, Dr. Rachida Bahbah, and Pr. El Mostapha Rakib: Investigation, Supervision, Conceptualization, Methodology, Validation, Revision and Editing.
Availability of Data
The data used in this research is available upon request from the authors (Dr. Oussama Aazzane, and Pr. Souad Mojahidi).
Figures and Tables
References
- Mazin Saleem Salman, Antibiotic Resistance of Bacteria Isolated in Urinary Tract Infections, J Contemp Med Sci, March-April 2024: 163–166
- Lei Huang, Chenwei Huang, Yan Yan, Liying Sun, Haixia L. Urinary Tract Infection Etiological Profiles and Antibiotic Resistance Patterns Varied Among Different Age Categories: A Retrospective Study From a Tertiary General Hospital During a 12-Year Period. Front Microbiol. January 2022. doi.org/10.3389/ fmicb.2021.813145i
- Solomon Wireko, Gifty Ngmaakan, Doreen Dwomoh et al. Regional Burden of Urinary Tract Infection, Its Aetiologies, and Antibiotic Resistance Patterns, 2020– 2023: A Retrospective Study. Health Science Reports, 2025. https://doi.org/10.1002/hsr2.71503
- Xiaofang Xu, Yuanfang Wang, Ning Li et al. Uropathogen profiles and their antimicrobial resistance patterns in patients: a three-year retrospective study in Sichuan region. Front. Public Health. February 2025. doi. org/10.3389/fpubh.2025.1493980
- Pedro Reyes-Martinez, Erick Sierra-Diaz, Pablo Cesar Ortiz-Lazareno et al. Microbiological profile and epidemiological perspective on urinary tract infections (UTIs) in a tertiary medical center in Western Mexico. Front. Microbiol. January 2026. doi.org/10.3389/ fmicb.2026.1734551
- Peter Farag , Hamzah Albulushi, Mohammed Eskembaji, et al. Prevalence and antibiotic resistance profile of UTI-causing uropathogenic bacteria in diabetics and non-diabetics at the Maternity and Children Hospital in Jeddah, Saudi Arabia. Front. Microbiol, November 2024. doi.org/10.3389/fmicb.2024.1507505
- Jingru Zhang, Shengyuan Wen, Liqing Chen, et al. Analysis of the microbial spectrum of urinary tract infections and antibiotic resistance of UPEC in Central Inner Mongolia, China. Front. Microbiol. September 2025. doi.org/10.3389/fmicb.2025.1599902
- Sipei Wang, Sheng Zhao, Tinghua Ye, et al. Comparison of antibiotic resistance and molecular characteristics of Escherichia coli isolated from patients with UTI, ASB, and uropathic bloodstream infection. Front. Med, December 2025. doi.org/10.3389/fmed.2025.1678401
- Xinwei Li, Yuanpeng Zhang, Wen Xiao, et al. Causative organisms of urinary tract infections and their drug sensitivity: an analysis from various aspects. Front. Public Health. October 2025. doi.org/10.3389/ fpubh.2025.1487721
- Mourad Chikhaoui, Rachid Lotfi, Ahmed Chetoui,et al. Epidemiology of Enterobacteriaceae uropathogenic strains and resistant to antibiotics in the clinical laboratory of the regional hospital of Beni Mellal, Morocco. International Journal of Biology Sciences. 2023. DOI: 10.33545/26649926.2023.v5.i2a.164
- Mohamed Kettani Halabi, Fatima Azzahra Lahlou, Idrissa Diawara, et al. Antibiotic Resistance Pattern of Extended Spectrum Beta Lactamase Producing Escherichia coli Isolated From Patients With Urinary Tract Infection in Morocco. Front Cell Infect Microbiol. 2021. doi: 10.3389/ fcimb.2021.720701
- Kitaba AA, Bonger ZT, Beyene D, et al. Antimicrobial resistance trends in clinical Escherichia coli and Klebsiella pneumoniae in Ethiopia. Afr J Lab Med. 2024. doi.org/10.4102/ajlm.v13i1.2268
- Elmostafa Benaissa, Elmehdi Belouad, Youness Mechal, el al. Multidrug-resistant community-acquired urinary tract infections in a northern region of Morocco: epidemiology and risk factors. Germs. 2021 . doi: 10.18683/germs.2021.1291
- Amelia Williams-Walker et al. Prevalence of antimicrobial resistance in acute community-acquired urinary tract infections in Sub-Saharan Africa: a systematic review. JAC-Antimicrobial Resistance. 2025. DOI:10.1093/ jacamr/dlaf230.064
- Solomon Bayaba , Raspail Carrel Founou, et al. High prevalence of multidrug resistant and extendedspectrum β-lactamase-producing Escherichia coli and Klebsiella pneumoniae isolated from urinary tract infections in the West region, Cameroon. BMC Infect Dis. 2025. doi: 10.1186/s12879-025-10483-8
- Jennifer Kranz, Riccardo Bartoletti, Franck Bruyère, et al. European Association of Urology Guidelines on Urological Infections: Summary of the 2024 Guidelines. Eur Urol. 2024. doi: 10.1016/j.eururo.2024.03.035
This is a text version generated from the article. For the formatted version of record (with original tables & figures), download the PDF →