Full Text Hide / show
Background
: Heterotopic ossification (HO) is characterized by the formation of mature lamellar bone in soft tissues and periarticular structures. Clinically, it may lead to pain, joint stiffness, mechanical block, reduced range of motion, and functional impairment. Although surgical excision is indicated in symptomatic and function-limiting cases, postoperative recurrence remains a relevant concern, particularly in high-risk patients and in anatomical sites other than the hip. Objective: To evaluate functional outcomes, postoperative complications, and recurrence rates in patients with symptomatic HO treated with open surgical excision followed by immediate postoperative prophylactic radiotherapy. Methodology: This retrospective institutional case series included patients diagnosed with symptomatic HO who underwent open surgical excision followed by postoperative external-beam radiotherapy.
Demographic characteristics, etiology, anatomical site, surgical and radiotherapyrelated variables, functional outcomes, complications, and recurrence were analyzed descriptively. Results: Five patients were included, comprising four males and one female, with a median age of 35 years, ranging from 18 to 52 years. Seven anatomical sites were treated: four elbows, two hips, and one shoulder. The etiologies included neurogenic, autoimmune/inflammatory, posttraumatic, and postoperative causes of HO. All treated sites received a single 8 Gy fraction of postoperative radiotherapy using 6 MV photons delivered with three-dimensional conformal radiotherapy (3D-CRT) within 24 hours after surgery. Functional improvement was observed in all treated sites, including increased range of motion, pain relief, improvement in gait or upper-limb function, and restoration of activities of daily living.
No cases of infection, wound-related complications, neurovascular injury, pathological fracture, radiotherapy-related toxicity, need for reintervention, or clinical or radiographic recurrence were observed during follow-up. Conclusion: Open surgical excision combined with immediate single-fraction prophylactic radiotherapy was feasible, safe, and associated with favorable functional outcomes in this case series. These findings support open surgical excision combined with immediate postoperative radiotherapy as a feasible multimodal strategy for selected patients with symptomatic HO. Keywords: Heterotopic ossification; surgical excision; prophylactic radiotherapy; orthopedic surgery; functional outcomes; recurrence.
Introduction
Heterotopic ossification (HO) is characterized by the abnormal formation of mature lamellar bone within soft tissues, including muscles and periarticular structures [1]. While it can affect various anatomical regions, the hip and elbow are most frequently involved in clinical practice [2]. The clinical presentation ranges from incidental radiographic findings to severe symptomatic disease causing pain, local inflammation, mechanical blocks, and significant functional impairment [3]. Its etiology is multifactorial, with acquired forms commonly linked to trauma, orthopedic surgery, burns, and prolonged immobilization [4]. Neurogenic HO—following traumatic brain injury, spinal cord injury, or stroke—often involves large joints and carries a higher risk of functional compromise and recurrence [5]. Similarly, post-traumatic and postoperative forms around the elbow are particularly debilitating, as even moderate restrictions in flexion-extension or rotation severely impact activities of daily living [6].
Pathophysiologically, HO arises from the dysregulated osteogenic differentiation of mesenchymal progenitor cells triggered by tissue injury and inflammation [7]. Signaling pathways, particularly bone morphogenetic proteins (BMP) and Wnt/β-catenin, drive this aberrant differentiation into osteoblastic lineages [8]. In this context, prophylactic radiotherapy acts by inhibiting the proliferation and osteogenic differentiation of these progenitor cells during the early postoperative period, effectively mitigating the probability of recurrent ectopic bone formation following surgical manipulation [9]. Managing symptomatic HO remains a clinical challenge. While conservative measures may suffice for asymptomatic or mildly symptomatic lesions, surgical excision is generally indicated for persistent pain, mechanical limitation, progressive stiffness, or severe functional impairment refractory to nonoperative care [10].
However, isolated surgical excision carries a significant recurrence risk, especially in patients with high-risk features such as neurogenic etiologies, extensive or multiple lesions, and a history of HO [11]. Consequently, multimodal prevention strategies—primarily nonsteroidal anti-inflammatory drugs and radiotherapy—are essential [11]. Single-fraction radiotherapy regimens of 8 Gy are well established, offering high efficacy, logistical simplicity, high adherence, and an acceptable toxicity profile [13]. Although the bulk of evidence supports its use after hip surgery [12], encouraging functional and radiographic outcomes have also been reported for non-hip sites, including the elbow [14]. Given the limited evidence regarding prophylactic radiotherapy for HO in non-hip anatomical sites and the high recurrence risk associated with surgically treated lesions, sharing institutional experiences is critical for guiding clinical decision-making.
Therefore, this retrospective case series aims to describe the clinical and surgical management of symptomatic HO across various anatomical sites treated with open excision and immediate postoperative prophylactic radiotherapy, with a focus on evaluating functional outcomes, complications, and recurrence rates.
Methodology
This Level IV retrospective observational case series was conducted through a comprehensive medical record analysis of patients treated at a specialized Orthopedics and Hand Surgery Service, in collaboration with a Radiotherapy Department, between March 2018 and November 2025. All data management procedures strictly complied with the Brazilian General Data Protection Law (LGPD), ensuring patient confidentiality via complete anonymization of identifiable information, restricting dataset access solely to the research team, and utilizing the extracted clinical data exclusively for scientific purposes. Eligibility for inclusion required patients to present with imaging-confirmed symptomatic heterotopic ossification (HO) associated with clinically significant functional impairment, a documented history of open surgical excision followed by postoperative radiotherapy, and a minimum clinical follow-up of one month.
Conversely, patients were excluded from the analysisiftheyhadincompletemedicalrecords,asymptomatic HO or lesions lacking functional limitation, or if postoperative radiotherapy was omitted from their therapeutic protocol. Data Collection Data were extracted from the reviewed medical records using a structured data collection form. Demographic, clinical, surgical, and radiotherapy-related variables were collected, including age, sex, etiology and anatomical site of HO, surgical approach, intraoperative findings, radiotherapy parameters, postoperative range of motion, pain progression, complications, recurrence, and need for reintervention. Surgical and Radiotherapy Protocols AllpatientsunderwentopensurgicalexcisionofHO.Thesurgical approach was selected according to the anatomical site, extent of ossification, degree of functional limitation, and relationship of the ectopic bone with adjacent neurovascular structures. Elbow procedures were performed through posterior or curvilinear anterior approaches, allowing adequate exposure, careful neurovascular protection, neurolysis when indicated, andcapsulotomyorarthrotomywhenrequired.Hipprocedures were performed using anterior Smith-Petersen or posterior Moore approaches, with marginal resection of the heterotopic bone and intraoperative assessment of joint mobility.
Shoulder procedures were managed through a posterior approach, with osteotomy performed when necessary. The main surgical objectives were removal of the mechanical block, restoration of passive range of motion, preservation of neurovascular structures, and minimization of additional soft-tissue trauma. Postoperative prophylactic external-beam radiotherapy was initiated within the first 24 hours after surgery. According to the institutional protocol, treatment consisted of a single fraction of 8 Gy delivered with 6 MV photons using threedimensional conformal radiotherapy (3D-CRT). The target volume encompassed the surgical bed with a 2 to 3 cm margin, with the objective of adequately covering the region at risk for recurrence while minimizing radiation exposure to adjacent healthy tissues.
Follow-up and Outcomes
Follow-up consisted of serial clinical and radiographic assessments. Clinical evaluations were performed at 15 days, 1 month, 3 months, and 6 months after surgery, and annually thereafter when available. These assessments focused on functional recovery, pain, range of motion, and return to activities of daily living.Radiographic assessments were performed at 1, 3, and 6 months postoperatively, with annual imaging obtained when clinically indicated. Computed tomography was reserved for cases of suspected recurrence or inconclusive radiographic findings.The primary outcomes were functional improvement and recurrence of HO. Functional improvement was assessed based on rangeof-motion gain, pain reduction, and resumption of daily activities. Recurrence was defined as new clinically relevant or radiographically evident bone formation within the surgical bed.Secondary outcomes included acute and late surgical complications, radiotherapy-related toxicity, pathological fractures, neurovascular injury, wound complications, and need for reintervention.
Statistical Analysis
Given the retrospective design and small sample size, data were analyzed descriptively. Continuous variables were summarized as medians and ranges, whereas categorical variables were reported as absolute and relative frequencies.
Results
Five patients met the inclusion criteria, comprising four males and one female, with a median age of 35 years, ranging from 18 to 52 years. A total of seven anatomical sites were surgically treated. The elbow was the most frequently involved region, accounting for four treated sites, followed by the hip in two sites and the shoulder in one site. The etiological profile was heterogeneous and included neurogenic, autoimmune/ inflammatory,post-traumatic,andpostoperativecausesofHO. Theclinicalanddemographiccharacteristicsofthepatientsare presented in Table 1. Preoperative radiographic evidence of HO was identified in six of the seven treated anatomical sites. The only exception was the shoulder in Case 3, which did not show preoperative HO before its subsequent development.
This lesion was considered a de novo manifestation in a distinct anatomical region, probably related to the patient’s underlying risk profile, rather than recurrence within the previously treated elbow surgical bed. All patients underwent open surgical excision followed by immediate postoperative prophylactic radiotherapy in accordance with the institutional protocol. Across all seven treated sites, external-beam radiotherapy was delivered within 24 hours after surgery as a single 8 Gy fraction, using 6 MV photons and 3D-CRT. The target volume encompassed the surgical bed. Table 1. Clinical and demographic characteristics of patients with heterotopic ossification. Case Sex Age Etiology Treated anatomical site(s) Preoperative HO Follow-up 1 Female 40 years Neurogenic, after stroke Left elbow and left hip Yes, both sites 9 months 2 Male 28 years Inflammatory/autoimmune, systemic lupus erythematosus Right hip Yes 8 months 3 Male 35 years Post-traumatic, after olecranon fracture Left elbow and left shoulder Yes, in the elbow; absent in the shoulder prior to subsequent development 18 months 4 Male 52 years Postoperative, after long head of biceps repair Left elbow Yes 3 months 5 Male 18 years Post-traumatic, after elbow fracture and prolonged immobilization Left elbow Yes 1 month and 5 days Legend: HO = heterotopic ossification.
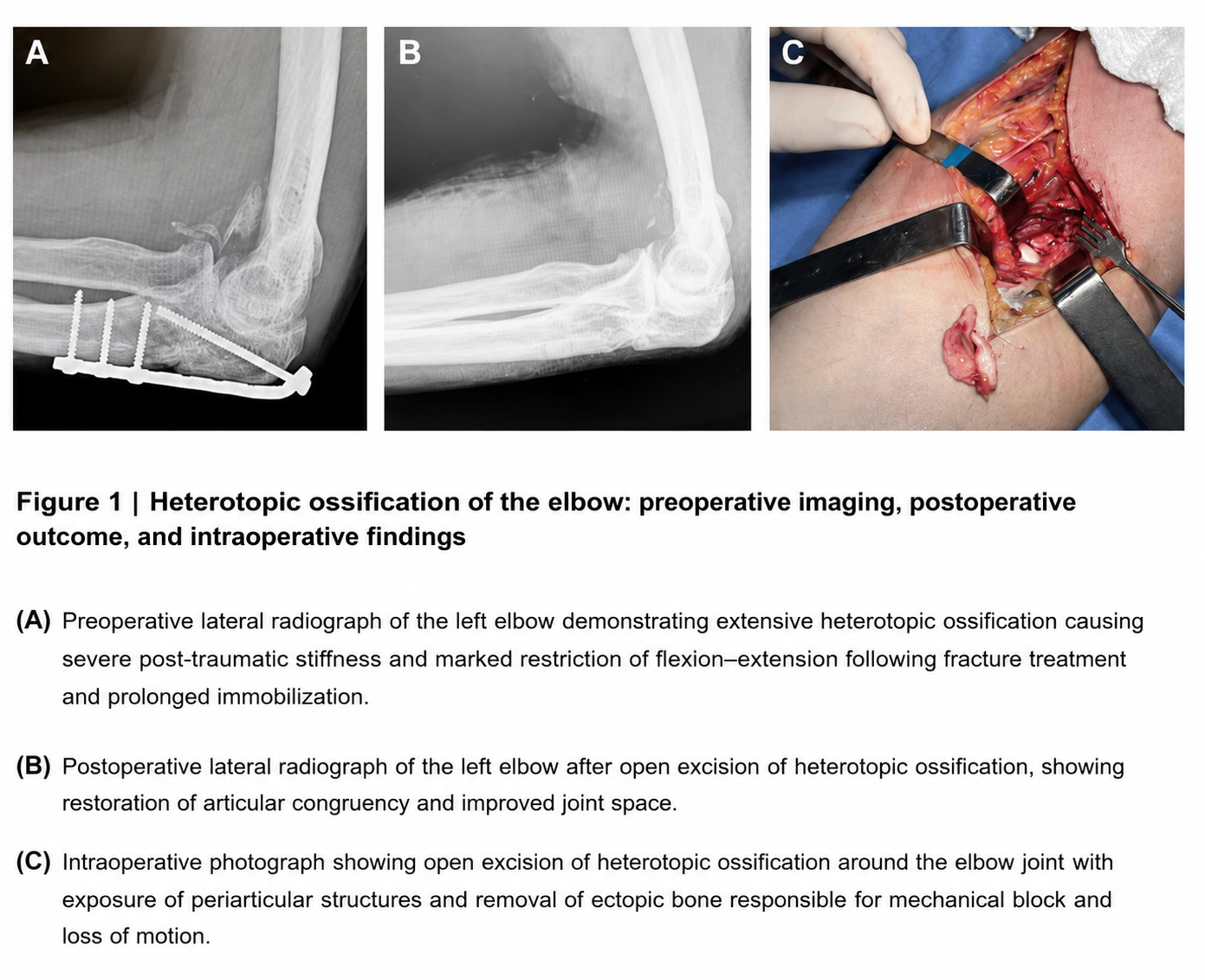
Figure 1 illustrates a representative case of post-traumatic HO of the elbow. The preoperative lateral radiograph demonstrates extensive ectopic bone formation associated with severe stiffness and marked restriction of flexion–extension. The postoperative radiograph shows improved joint space and restoration of articular congruency after surgical excision. The intraoperative image highlights the exposure of periarticular structures and removal of ectopic bone responsible for the mechanical block and functional limitation. Figure 1. Heterotopic ossification of the elbow: preoperative imaging, postoperative outcome, and intraoperative findings. Postoperative outcomes are summarized in Table 2. Functional improvement was observed in all treated anatomical sites. Elbow procedures resulted in recovery of flexion–extension and/or pronation–supination. Hip procedures were associated with improved flexion, abduction, rotation, correction of contracture, and better gait pattern.
The shoulder procedure resulted in complete pain resolution and increased range of motion. Case 1 showed excellent functional recovery after open excision of HO in the left elbow and left hip, with elbow flexion improving to 130°, restoration of supination, and improved hip mobility with contracture correction. Case 2 demonstrated a good functional outcome after right hip excision, with improvement in hip flexion, abduction, rotation, and gait. Case 3 achieved excellent recovery after treatment of the left elbow and left shoulder, with complete restoration of elbow flexionextension and resolution of shoulder pain. Case 4 showed significant improvement in pronation-supination and global elbow function. Case 5, despite having the shortest follow-up period, demonstrated objective improvement in elbow mobility, with flexion increasing from 68° to 96° and the extension deficit decreasing from 50° to 28°.
Table 2. Treatment protocol, functional outcomes, complications, and recurrence. Case Surgical treatment Radiotherapy protocol Functional outcome Complications Recurrence 1 Open excision of left elbow and left hip HO 8 Gy, single fraction, <24 h after each procedure Excellent; elbow flexion improved to 130°, supination was restored, and hip mobility improved with contracture correction None No 2 Open excision of right hip HO 8 Gy, single fraction, <24 h postoperatively Good; improvement in hip flexion, abduction, rotation, and gait pattern None No 3 Open excision of left elbow and left shoulder HO 8 Gy, single fraction, <24 h after each procedure Excellent; complete elbow flexion–extension was restored, and shoulder pain resolved with improved range of motion None No 4 Open excision of left elbow HO 8 Gy, single fraction, <24 h postoperatively Good; significant improvement in pronation– supination and global elbow function None No 5 Open excision of left elbow HO 8 Gy, single fraction, <24 h postoperatively Good; flexion improved from 68° to 96°, extension deficit decreased from 50° to 28°, with marked mobility gain None No Legend: HO=heterotopic ossification; Gy=gray; h=hours.
Thecombinedsurgicalandradiotherapeuticapproachwaswell tolerated. No acute or late complications were documented during the available follow-up period. Specifically, there were no cases of infection, wound dehiscence, neurovascular injury, radiotherapy-related toxicity, pathological fracture, paradoxical stiffness, or need for reintervention. No clinical or radiographic recurrence was observed in any of the seven treated anatomical sites during follow-up. Therefore, the overall recurrence rate was 0%. Serial clinical and radiographic assessments did not identify new ectopic bone formation within the surgical beds. The shoulder lesion observed in Case 3 was interpreted as a de novo HO event in a different anatomical region, rather than local recurrence of the previously treated elbow lesion.
Discussion
This retrospective case series evaluated five patients with symptomatic HO, corresponding to seven surgically treated anatomical sites. The cohort was clinically heterogeneous, including neurogenic, autoimmune/inflammatory, posttraumatic, and postoperative etiologies, with involvement of four elbows, two hips, and one shoulder. Despite this heterogeneity, all patients were managed using the same multimodal strategy: open surgical excision followed by immediate postoperative prophylactic external-beam radiotherapy, delivered as a single 8 Gy fraction with 6 MV photons using 3D-CRT within 24 hours after surgery. The main findings were functional improvement in all treated anatomical sites, absence of acute or late complications, no need for reintervention, and no clinical or radiographic recurrence during the available follow-up period.
These results suggest that, in carefully selected patients with symptomatic and function-limiting HO, open excision combined with immediate postoperative radiotherapy may represent a feasible and safe therapeutic approach. This is particularly relevant in cases in which ectopic bone formation causes mechanical block, pain, stiffness, gait impairment, or substantial limitation of activities of daily living [1-6]. The biological rationale for this combined approach is supported by the pathophysiology of HO. HO results from an abnormal osteogenic process within soft tissues, mediated by inflammatory stimuli, mesenchymal progenitor-cell activation, osteogenic differentiation, and local osteoinductive signaling. Although surgical excision removes mature ectopic bone and restores joint mobility, the surgical trauma itself may reactivate inflammatory and osteogenic pathways, creating a biological environment favorable to recurrence.
In this context, immediate postoperative radiotherapy aims to inhibit the early proliferative phase of osteoprogenitor cells within the surgical bed before mature ectopic bone can reform. The use of a single 8 Gy fraction within the first 24 postoperative hours is consistent with commonly accepted prophylactic regimens and offers practical advantages, including logistical simplicity, treatment reproducibility, patient adherence, and early initiation or continuation of rehabilitation [7-14]. The present series also highlights the clinical relevance of patient selection. All included cases had symptomatic disease with relevant functional limitation, and treatment was directed toward the removal of a mechanical block or restoration of motion in functionally important joints. Functional improvement was observed across all treated sites, regardless of etiology.
This finding suggests that the indication for surgery and adjuvant radiotherapy should be primarily guided by the clinical impact of the lesion, the degree of functional impairment, the anatomical relationship of the ectopic bone with neurovascular structures, and the risk of recurrence, rather than by etiology alone. Case 1 involved a 40-year-old female patient with neurogenic HO after stroke, affecting both the left elbow and left hip. This case represents a high-risk biological phenotype, since neurogenic HO is frequently associated with intense inflammatory activation, prolonged immobilization, spasticity, and extensive periarticular ossification. The involvement of two major functional joints further increased the clinical burden. After open excision and postoperative radiotherapy, the patient achieved an excellent outcome, with elbow flexion improving to 130°, restoration of supination, and improved hip mobility with correction of contracture.
The absence of recurrence after 9 months is clinically relevant, as neurogenic cases are generally considered more prone to recurrence and functional deterioration. In this context, the combined protocol appears to have preserved the mobility obtained intraoperatively and may have reduced the likelihood of renewed ectopic bone formation in both treated sites [15-21]. Case 2 was a 28-year-old male patient with autoimmune/ inflammatory HO associated with systemic lupus erythematosus, affecting the right hip. This case is noteworthy because systemic inflammatory conditions may contribute to abnormal tissue repair and pathological ossification. The hip lesion produced relevant functional impairment, particularly involving flexion, abduction, rotation, and gait. Following open excision and immediate radiotherapy, the patient demonstrated improved hip mobility and gait pattern, without complications or recurrence at 8 months.
These findings support the potential role of local radiotherapy prophylaxis even in patients with systemic risk factors, provided that the treatment field adequately covers the surgical bed and that the indication is based on clinically meaningful limitation [15-21]. Case 3 involved a 35-year-old male patient with post-traumatic HO after olecranon fracture, initially affecting the left elbow and later the left shoulder. This case had the longest followup period, reaching 18 months. The elbow lesion exemplifies a typical post-traumatic pattern, in which periarticular ectopic bone causes severe stiffness and mechanical restriction in a joint highly dependent on preserved range of motion. As illustrated in Figure 1, preoperative imaging demonstrated extensive ectopic bone formation associated with marked limitation of flexion-extension, whereas postoperative imaging showed restoration of joint congruency and improved articular space after excision.
Clinically, complete restoration of elbow flexion-extension was achieved, with no recurrence within the surgical bed. The subsequent shoulder involvement in Case 3 should not be interpreted as local recurrence, because it occurred in a different anatomical region. Rather, it was considered a de novo HO event, probably related to the patient’s individual predisposition to ectopic bone formation. Its successful treatment, with complete pain resolution and improved range of motion, suggests that the same multimodal principles may be applicable to less common anatomical sites when the lesion is symptomatic and functionally relevant. This case reinforces the importance of distinguishing true recurrence within the operated field from new HO in another joint, especially in patients with persistent biological susceptibility [22-30].
Case 4 was a 52-year-old male patient with postoperative HO after long head of biceps repair, affecting the left elbow. This case demonstrates that clinically significant HO may occur not only after major trauma but also after orthopedic procedures involving periarticular soft-tissue injury. The main functional impairment was related to pronation-supination and global elbow function. After excision and single-fraction postoperative radiotherapy, the patient showed significant improvement, without wound complications, neurovascular injury, radiotherapy-related toxicity, or recurrence during the 3-month follow-up. Although the follow-up period remains limited, the early postoperative course supports the safety of the protocol and emphasizes the importance of timely intervention before irreversible functional compromise becomes established [22-30]. Case5involvedan18-year-oldmalepatientwithpost-traumatic HO after elbow fracture and prolonged immobilization.
This case deserves particular attention because the patient was the youngest in the cohort and had the shortest follow-up period, corresponding to 1 month and 5 days. Despite this limitation, objective functional improvement was already evident, with elbow flexion increasing from 68° to 96° and the extension deficit decreasing from 50° to 28°. These findings indicate meaningful early recovery of motion in a previously stiff elbow limited by mechanical block. However, longer follow-up is essential to determine the durability of functional gains, monitor late recurrence, and identify possible delayed adverse events. In younger patients, the indication for radiotherapy must be especially individualized, balancing the functional consequences of recurrence against the theoretical long-term risks of radiation exposure [31-37].
When the cohort is analyzed as a whole, several relevant patterns emerge. First, functional improvement occurred in all treated sites, supporting the clinical value of addressing symptomatic HO when there is clear mechanical or functional limitation. Second, the elbow was the most frequently treated anatomical region, reinforcing the relevance of this joint in HO-related disability. Because even modest losses of elbow motion may significantly affect activities of daily living, restoration of flexion-extension and forearm rotation represents an important therapeutic goal. Third, the absence of recurrence in seven treated sites suggests that immediate postoperative radiotherapy may contribute to maintaining the gains obtained by surgical excision. Fourth, the absence of infection, wound complications, neurovascular injury, pathological fracture, radiotherapy-related toxicity, paradoxical stiffness, and reintervention supports the favorable safety profile of the standardized protocol used in this series [31-37].
The favorable results observed may be partly explained by careful surgical planning and standardized radiotherapy delivery. Surgical approaches were selected according to anatomical site, extent of ossification, and proximity to neurovascular structures. The main objectives were removal of the mechanical block, preservation of neurovascular structures, restoration of passive motion, and minimization of additional soft-tissue trauma. Radiotherapy was delivered within a narrow postoperative window, targeting the surgical bed with a 2 to 3 cm margin. This field design sought to cover the area at risk for recurrence while limiting exposure to adjacent healthy tissues. Nevertheless, the use of radiotherapy for benign disease requires individualized risk-benefit analysis. Although the theoretical risk of radiation-induced malignancy is considered very low with modern low-dose prophylactic regimens, it remains a relevant consideration, particularly in young patients, individuals requiring treatment at multiple sites, and patients with long life expectancy.
Therefore, postoperative radiotherapy should not be considered a universal indication after HO excision. Instead, it should be reserved for selected patients in whom the risk of recurrence and the expected functional consequences justify adjuvant prophylaxis [31-37]. This study has important limitations. Its retrospective design, small sample size, absence of a control group, etiological heterogeneity, and variable follow-up periods limit the strength of causal inference. Validated functional outcome scores were not systematically applied, and some patients, particularly Case 5, had short follow-up. In addition, the retrospective nature of the study may have introduced selection bias. Therefore, although the absence of recurrence and complications is encouraging, these findings should be interpreted with caution.
From a practical perspective, this multimodal protocol may be particularly useful in high-risk patients with function-limiting HO involving anatomically complex joints, especially when recurrence could lead to substantial disability. Despite these limitations, the case-by-case analysis provides clinically useful information. The results indicate that open excision followed by immediate single-fraction postoperative radiotherapy was associated with consistent functional improvement, absence of recurrence, and no documented complications across different etiologies and anatomical sites. These findings support the use of a standardized multimodal approach in selected patients with symptomatic HO, including non-hip sites such as the elbow and shoulder. Future prospective studies with larger cohorts, longer followup, standardized functional assessment, and comparative groups are needed to better define the magnitude of benefit, optimal patient selection, and long-term safety of this strategy.
Conclusion
This retrospective case series showed that open surgical excision followed by immediate postoperative prophylactic radiotherapy was feasible, safe, and associated with favorable outcomes in patients with symptomatic HO. Five patients were included, corresponding to seven treated anatomical sites: four elbows, two hips, and one shoulder. Despite the etiological heterogeneity, including neurogenic, autoimmune/ inflammatory, post-traumatic, and postoperative causes, functional improvement was observed in all treated sites. The surgical procedure contributed to removal of the mechanical block and restoration of joint function. Elbow procedures resulted in improved flexion-extension and/or pronation-supination, hip procedures were associated with better mobility, contracture correction, and gait improvement, and the shoulder procedure resulted in pain resolution and increased range of motion.
In the youngest patient, despite the short follow-up, objective improvement was already observed, with elbow flexion increasing from 68° to 96° and the extension deficit decreasing from 50° to 28°. Postoperative radiotherapy was delivered uniformly in all treated sites as a single 8 Gy fraction using 6 MV photons and 3D-CRT within 24 hours after surgery. This standardized protocol was well tolerated, with no documented cases of infection, wound complication, neurovascular injury, pathological fracture, radiotherapy-related toxicity, paradoxical stiffness, or need for reintervention. No clinical or radiographic recurrence was observed during the available follow-up period, resulting in an overall recurrence rate of 0% among the seven treated anatomical sites. These findings support the use of open excision combined with immediate single-fraction prophylactic radiotherapy as a potential multimodal strategy for selected patients with symptomatic and function-limiting HO, including nonhip sites such as the elbow and shoulder.
However, due to the retrospective design, small sample size, etiological heterogeneity, and variable follow-up duration, these results should be interpreted with caution. Prospective studies with larger cohorts, longer follow-up, standardized functional assessment, and comparative groups are needed to confirm the effectiveness, safety, and durability of this approach.
Figures and Tables
| Case | Sex | Age | Etiology | Treated anatomical site(s) | Preoperative HO | Follow-up |
|---|---|---|---|---|---|---|
| 1 | Female | 40 years | Neurogenic, after stroke | Left elbow and left hip | Yes, both sites | 9 months |
| 2 | Male | 28 years | Inflammatory/autoimmune, systemic lupus erythematosus | Right hip | Yes | 8 months |
| 3 | Male | 35 years | Post-traumatic, after olecranon fracture | Left elbow and left shoulder | Yes, in the elbow; absent in the shoulder prior to subsequent development | 18 months |
| 4 | Male | 52 years | Postoperative, after long head of biceps repair | Left elbow | Yes | 3 months |
| 5 | Male | 18 years | Post-traumatic, after elbow fracture and prolonged immobilization | Left elbow | Yes | 1 month and 5 days |
| Case | Surgical treatment | Radiotherapy protocol | Functional outcome | Complications | Recurrence |
|---|---|---|---|---|---|
| 1 | Open excision of left elbow and left hip HO | 8 Gy, single fraction, <24 h after each procedure | Excellent; elbow flexion improved to 130°, supination was restored, and hip mobility improved with contracture correction | None | No |
| 2 | Open excision of right hip HO | 8 Gy, single fraction, <24 h postoperatively | Good; improvement in hip flexion, abduction, rotation, and gait pattern | None | No |
| 3 | Open excision of left elbow and left shoulder HO | 8 Gy, single fraction, <24 h after each procedure | Excellent; complete elbow flexion–extension was restored, and shoulder pain resolved with improved range of motion | None | No |
| 4 | Open excision of left elbow HO | 8 Gy, single fraction, <24 h postoperatively | Good; significant improvement in pronation– supination and global elbow function | None | No |
| 5 | Open excision of left elbow HO | 8 Gy, single fraction, <24 h postoperatively | Good; flexion improved from 68° to 96°, extension deficit decreased from 50° to 28°, with marked mobility gain | None | No |
References
- Kaplan FS, Glaser DL, Hebela N, Shore EM. Heterotopic ossification. J Am Acad Orthop Surg. 2004;12(2):116- 125. doi:10.5435/00124635-200403000-00007
- Sylvester PL, Decker S, Kragh JF Jr, Hsu JR. Prevention and management of heterotopic ossification. J Am Acad Orthop Surg. 2009;17(4):245-253. doi:10.5435/00124635-200904000-00006
- Ranganathan K, Loder S, Agarwal S, et al. Heterotopic ossification: basic-science principles and clinical correlates. J Bone Joint Surg Am. 2015;97(13):1101- 1111. doi:10.2106/JBJS.N.01056
- Garland DE. A clinical perspective on common forms of acquired heterotopic ossification. Clin Orthop Relat Res. 1991;(263):13-29. doi:10.1097/00003086-199102000- 00003
- Vanden Bossche L, Vanderstraeten G. Heterotopic ossification: a review. J Rehabil Med. 2005;37(3):129- 136. doi:10.1080/16501970510027628
- Viola RW, Hastings H. Treatment of ectopic ossification abouttheelbow.ClinOrthopRelatRes.2000;(370):65-86.
- Shore EM, Xu M, Feldman GJ, et al. A recurrent mutation in the BMP type I receptor ACVR1 causes inherited and sporadic fibrodysplasia ossificans progressiva. Nat Genet. 2006;38(5):525-527. doi:10.1038/ng1783
- Brooker AF, Bowerman JW, Robinson RA, Riley LH Jr. Ectopic ossification following total hip replacement: incidence and a method of classification. J Bone Joint Surg Am. 1973;55(8):1629-1632.
- Chao ST, Lee SY, Borden LS, Joyce MJ, Krebs VE, Suh JH. External beam radiation helps prevent heterotopic bone formation in patients with a history of heterotopic ossification. J Arthroplasty. 2006;21(5):731-736. doi:10.1016/j.arth.2005.08.014
- Hastings H 2nd, Graham TJ. The classification and treatment of heterotopic ossification about the elbow and forearm. Hand Clin. 1994;10(3):417-437.
- Seegenschmiedt MH, Keilholz L, Martus P, et al. Prevention of heterotopic ossification about the hip: final results of two randomized trials in 410 patients using either preoperative or postoperative radiation therapy. Int J Radiat Oncol Biol Phys. 1997;39(1):161- 171. doi:10.1016/S0360-3016(97)00285-X
- Lo TC, Healy WL, Covall DJ, et al. Heterotopic bone formation after hip surgery: prevention with single-dose postoperativehipirradiation.Radiology.1988;168(3):851- 854. doi:10.1148/radiology.168.3.3136510
- Patel AB, Tzou KS, Single M, et al. Radiation therapy prophylaxis for heterotopic ossification in non-hip sites. J Cancer Ther. 2018;9(1):1-8. doi:10.4236/jct.2018.91001
- Balboni TA, Gobezie R, Mamon HJ. Heterotopic ossification: pathophysiology, clinical features, and the role of radiotherapy for prophylaxis. Int J Radiat Oncol Biol Phys. 2006;65(5):1289-1299. doi:10.1016/j ijrobp.2006.03.053
- Ackerman I, Esler C. Prophylaxis against heterotopic ossification after total hip replacement. Curr Opin Rheumatol. 2007;19(2):168-173. doi:10.1097/ BOR.0b013e328011c97d
- Vavken P, Castellani L, Sculco TP. Prophylaxis of heterotopic ossification of the hip: systematic review and meta-analysis. Clin Orthop Relat Res. 2009;467(12):3283- 3289. doi:10.1007/s11999-009-0924-5
- Ayers DC, Pellegrini VD Jr, Evarts CM. Prevention of heterotopic ossification in high-risk patients by radiation therapy. Clin Orthop Relat Res. 1991;(263):87-93.
- Coventry MB, Scanlon PW. The use of radiation to discourage ectopic bone: a nine-year study in surgery about the hip. J Bone Joint Surg Am. 1981;63(2):201-208. doi:10.2106/00004623-198163020-00004
- Gregoritch SJ, Chadha M, Pellegrini VD Jr, Rubin P, Kantorowitz DA. Randomized trial comparing preoperative versus postoperative irradiation for prevention of heterotopic ossification following prosthetic total hip replacement: preliminary results. Int J Radiat Oncol Biol Phys. 1994;30(1):55-62. doi:10.1016/0360-3016(94)90519-3
- Seegenschmiedt MH, Makoski HB, Micke O, German Cooperative Group on Radiotherapy for Benign Diseases. Radiation prophylaxis for heterotopic ossification about the hip joint: a multicenter study. Int J Radiat Oncol Biol Phys. 2001;51(3):756-765. doi:10.1016/ S0360-3016(01)01640-6
- Ring D, Jupiter JB. Operative release of complete ankylosis of the elbow due to heterotopic bone in patients without severe injury of the central nervous system. J Bone Joint Surg Am. 2003;85(5):849-857. doi:10.2106/00004623-200305000-00011
- Shehab D, Elgazzar AH, Collier BD. Heterotopic ossification. J Nucl Med. 2002;43(3):346-353.
- Garland DE, O’Hollaren RM. Fractures and dislocations about the elbow in the head-injured adult. Clin Orthop Relat Res. 1982;(168):38-41. doi:10.1097/00003086- 198208000-00006
- Ippolito E, Formisano R, Farsetti P, Caterini R, Penta F. Excision for the treatment of periarticular ossification of the knee in patients who have a traumatic brain injury. J Bone Joint Surg Am. 1999;81(6):783-789. doi:10.2106/00004623-199906000-00005
- Schaeffer MA, Sosner J. Heterotopic ossification: treatment of established bone with radiation therapy. ArchPhysMedRehabil.1995;76(3):284-286.doi:10.1016/ S0003-9993(95)80617-2
- Childs HA 3rd, Cole T, Falkenberg ET, et al. A prospective evaluation of the timing of postoperative radiotherapy for preventing heterotopic ossification following traumatic acetabular fractures. Int J Radiat Oncol Biol Phys. 2000;47(5):1347-1352. doi:10.1016/S0360- 3016(00)00582-4
- Mourad WF, Ma JK, Packianathan S, et al. Clinically relevant heterotopic ossification after elbow surgery: a systematic review with a focus on post-traumatic elbow contracture. Arch Orthop Trauma Surg. 2014;134(12):1791-1798. doi:10.1007/s00402-014-2107-
- Sellers RS, Radiation Therapy Oncology Group. Heterotopic bone formation: a comprehensive review. J Bone Joint Surg Am. 2004;86(11):2543-2553.
- Konski A, Pellegrini V, Poulter C, et al. Randomized trial comparing single-dose versus fractionated irradiation for prevention of heterotopic bone: a preliminary report. Int J Radiat Oncol Biol Phys. 1990;18(5):1139- 1142. doi:10.1016/0360-3016(90)90450-X
- Liu JZ, Frisch NB, Barden RM, Rosenberg AG, Silverton CD, Galante JO. Heterotopic ossification prophylaxis after total hip arthroplasty: randomized trial of 400 vs 700 cGy. J Arthroplasty. 2017;32(4):1328-1334. doi:10.1016/j.arth.2016.10.030
- Neal BC, Rodgers A, Clark T, et al. A systematic survey of 13 randomized trials of non-steroidal anti-inflammatory drugs for the prevention of heterotopic bone formation after major hip surgery. Acta Orthop Scand. 2000;71(2):122-128. doi:10.1080/000164700317413076
- Pakos EE, Ioannidis JP. Radiotherapy versus nonsteroidal anti-inflammatory drugs for the prevention of heterotopic ossification after major hip procedures: a meta-analysis of randomized trials. Int J Radiat Oncol Biol Phys. 2004;60(3):888-895. doi:10.1016/j ijrobp.2003.11.015
- Ippolito E, Formisano R, Caterini R, Farsetti P, Penta F. Operative treatment of heterotopic hip ossification in patients with coma after brain injury. Clin Orthop Relat Res. 1999;(365):130-138.
- Edwards DS, Clasper JC. Heterotopic ossification: a systematic review. J R Army Med Corps. 2015;161(4):315- 321. doi:10.1136/jramc-2014-000277
- Ron E, Modan B, Boice JD Jr, et al. Tumors of the brain and nervous system after radiotherapy in childhood. N Engl J Med. 1988;319(16):1033-1039. doi:10.1056/ NEJM198810203191601
- Micke O, Seegenschmiedt MH, German Cooperative Group on Radiotherapy for Benign Diseases. Radiation therapy for benign diseases in Germany: current concepts and future perspectives. Strahlenther Onkol. 2002;178(4):179-186.
- Almangour W, Schnitzler A, Salga M, et al. Recurrence of heterotopic ossification after removal in patients with traumatic brain injury: a systematic review. Ann Phys Rehabil Med. 2016;59(4):263-269. doi:10.1016/j rehab.2016.03.009
This is a text version generated from the article. For the formatted version of record (with original tables & figures), download the PDF →