Full Text Hide / show
Introduction
Fragility fractures represent a major and growing public health concern worldwide, particularly among postmenopausal women, in whom the decline in estrogen levels significantly accelerates bone loss and compromises skeletal integrity. Osteoporosis, the underlying condition responsible for most fragility fractures, is characterized by reduced bone mineral density and deterioration of bone microarchitecture, predisposing individuals to fractures even after minimal trauma. Among postmenopausal women, common fracture sites include the hip, vertebrae, pelvis, and long bones, all of which are associated with substantial morbidity, reduced quality of life, and increased mortality. As global life expectancy continues to rise, the burden of osteoporotic fractures and their associated complications is expected to increase dramatically, placing additional strain on healthcare systems. [1] While the initial management of fragility fractures has been extensively studied, increasing attention is being directed toward the complications that arise during the healing process and recovery period. These complications include delayed union, nonunion, infection, fixation failure, refracture, chronic pain, and functional decline. Such adverse outcomes not only prolong hospitalization and rehabilitation but also significantly impact long-term independence and survival, particularly in elderly populations. Hip fractures, for instance, are associated with a one-year mortality rate of up to 20– 30%, emphasizing the critical need for effective management strategies that extend beyond the acute phase of care. [2] The pathophysiology of fracture complications in postmenopausal women is multifactorial. Estrogen deficiency leads to increased bone resorption and impaired bone formation, resulting in delayed healing and reduced biomechanical strength at fracture sites. [3] Additionally, age-related comorbidities, including diabetes, cardiovascular disease, and sarcopenia, further complicate recovery and increase the risk of adverse outcomes. [4] Nutritional deficiencies, particularly in calcium and vitamin D, along with reduced physical activity, also contribute to poor fracture healing and increased susceptibility to subsequent fractures. [5] Management of complications following fragility fractures requires a comprehensive and multidisciplinary approach. Pharmacological interventions play a central role, with antiresorptive agents such as bisphosphonates and denosumab, as well as anabolic agents like teriparatide, demonstrating efficacy in improving bone density and reducing fracture risk. [6] Hormone replacement therapy has also been shown to have beneficial effects in selected populations. In addition to pharmacotherapy, surgical management—including optimal timing of intervention and advanced fixation techniques—remains critical in minimizing complications such as implant failure and nonunion. [7]
Rehabilitation strategies are equally important in improving functional outcomes and reducing the risk of long-term disability. Early mobilization, physiotherapy, and structured exercise programs have been shown to enhance recovery, improve muscle strength, and decrease the incidence of frailty and falls. [8] Furthermore, healthcare system interventions such as fracture liaison services have emerged as effective models for coordinating post-fracture care, ensuring appropriate evaluation, treatment, and follow-up to prevent secondary fractures. Despite advances in the management of fragility fractures, significant gaps remain in the understanding and prevention of associated complications. Variability in clinical practice, limited adherence to treatment guidelines, and disparities in access to care continue to hinder optimal outcomes. Moreover, emerging therapies, including biologic agents and regenerative approaches, offer promising avenues but require further investigation through high-quality studies. [9] Given these challenges, there is a critical need to synthesize current evidence on the management of fracture-related complications in postmenopausal women. This study aims to systematically review and analyze recent literature to evaluate existing management strategies, identify key determinants of outcomes, and highlight future directions for research and clinical practice. By providing a comprehensive overview of current evidence, this work seeks to inform clinicians, researchers, and policymakers in developing effective interventions to reduce the burden of fragility fracture complications in this vulnerable population. [10] [11]
The primary objective of this study was to systematically evaluate and synthesize current evidence on the management of complications following fragility fractures in postmenopausal women, with the aim of improving clinical outcomes and informing future research directions. Specifically, the study sought to identify the most common complications associated with fragility fractures in this population and to assess the effectiveness of various management strategies. These included pharmacological interventions such as antiresorptive and anabolic therapies, as well as surgical approaches focusing on timing and fixation techniques to reduce complication rates. Additionally, the study aimed to analyze the role of rehabilitation and structured exercise programs in enhancing functional recovery and preventing long-term disability. The effectiveness of healthcare system interventions, including fracture liaison services and preventive screening programs, was also examined in relation to reducing secondary fractures. Furthermore, the study explored key risk factors associated with poor healing outcomes, including nonunion and infection, and aimed to highlight existing gaps in the literature while proposing directions for future research and clinical practice.
This study was conducted as a systematic review and metaanalysis in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines to ensure transparency, reproducibility, and methodological rigor in the identification, selection, and analysis of relevant studies. The literature search encompassed studies published between January 2022 and March 2026, thereby capturing the most recent and clinically relevant evidence on the management of complications following fragility fractures in postmenopausal women. Eligibility criteria were clearly defined prior to study selection. Studies were included if they involved postmenopausal women with fragility fractures and addressed complications such as nonunion, delayed union, infection, fixation failure, refracture, or mortality. Additionally, only studies evaluating management strategies—including pharmacological interventions, surgical approaches, rehabilitation programs, or healthcare system-based interventions—were considered. Eligible study designs included systematic reviews, metaanalyses, randomized controlled trials, cohort studies, and case–control studies, provided they were published in English within the specified time frame. Studies were excluded if they involved non-human subjects, were not specific to postmenopausal women, or did not report relevant outcomes related to fracture complications. Furthermore, case reports, editorials, and narrative reviews lacking sufficient clinical data were excluded, as were duplicate publications and studies with incomplete or insufficient data. This rigorous selection process ensured that only high- quality and relevant evidence was included in the analysis.
Methods
of Data Collection A comprehensive search strategy was applied across multiple databases, including PubMed, Scopus, Web of Science, Embase, and Google Scholar. Relevant keywords and Medical Subject Headings (MeSH) terms were used, such as “fragility fractures,” “postmenopausal women,” “osteoporosis,” “fracture complications,” “nonunion,” “infection,” and “fracture management.” Two independent reviewers screened titles and abstracts for eligibility, followed by full-text assessment. Discrepancies were resolved through discussion or consultation with a third reviewer. Data extraction was performed using a standardized form, capturing study characteristics, population details, interventions, outcomes, and key findings.
Analysis of Data
Data were analyzed using both qualitative and quantitative approaches. A descriptive synthesis was performed to summarize study characteristics, types of complications, and management strategies. For studies with comparable
outcomes, a meta-analysis was conducted using appropriate statistical models. Effect sizes such as risk ratios (RR), odds ratios (OR), and hazard ratios (HR) with 95% confidence intervals (CI) were calculated. Heterogeneity among studies was assessed using the I² statistic, with values above 50% indicating substantial heterogeneity. Where appropriate, subgroup analyses were performed based on type of intervention, fracture site, and study design. Publication bias was evaluated using funnel plots and statistical tests. Statistical analysis was conducted using standard software such as RevMan or STATA, ensuring robustness and reliability of findings.
Literature Review
Fragility fractures are a hallmark complication of osteoporosis and represent a major health burden among postmenopausal women worldwide. The decline in estrogen levels following menopause leads to accelerated bone resorption, reduced bone mineral density, and increased susceptibility to fractures even with minimal trauma. Hip, vertebral, and wrist fractures are among the most commonly reported, each associated with significant morbidity, mortality, and healthcare costs. [12] A growing body of literature has emphasized that the burden of fragility fractures extends beyond the initial injury, with complications during healing and recovery contributing substantially to adverse outcomes. Delayed union and nonunion are among the most frequently reported complications, particularly in osteoporotic bone where impaired remodeling and reduced vascularity hinder normal healing processes. [13] [14] Infection and sepsis following fractures, especially in surgically managed cases, represent another critical concern. Evidence suggests that elderly patients with fragility fractures are more vulnerable to postoperative infections due to weakened immune responses and prolonged hospital stays. [15] Fixation failure is another important complication in osteoporotic fractures. Reduced bone quality compromises the stability of implants, leading to loosening, displacement, or mechanical failure. [16] Refracture and subsequent fractures are also widely reported in postmenopausal women. A prior fragility fracture significantly increases the risk of future fractures, creating a cycle of recurrent injury and functional decline. [17] Pharmacological management plays a central role in reducing fracture risk and improving healing outcomes. Antiresorptive agents such as bisphosphonates and denosumab have been widely used to decrease bone resorption and prevent further bone loss. [18] More recently, anabolic agents such as teriparatide have gained attention for their ability to stimulate bone formation and enhance fracture healing, particularly in cases of delayed union or nonunion. [19] Hormone replacement therapy has also been explored as a treatment option, particularly in early postmenopausal
women. While effective in improving bone density, its use is often limited by concerns regarding long-term safety and associated risks. [20] Surgical management is a critical component in the treatment of fragility fractures, particularly for hip and vertebral fractures. Evidence consistently shows that early surgical intervention, especially within 24–48 hours for hip fractures, is associated with reduced complications, shorter hospital stays, and improved survival rates. [21] Rehabilitation and physical therapy are essential for restoring function and preventing long-term disability. Early mobilization has been shown to reduce complications such as deep vein thrombosis, muscle atrophy, and pneumonia. [22] Frailty is increasingly recognized as both a risk factor and an outcome of fragility fractures. Postmenopausal women who experience fractures often exhibit accelerated functional decline, loss of independence, and increased need for longterm care. [23] Fracture liaison services (FLS) have emerged as an effective healthcare model for improving post-fracture care. These multidisciplinary programs ensure that patients receive appropriate assessment, treatment, and follow-up,
significantly reducing the risk of secondary fractures. [24] Preventive strategies, including screening for osteoporosis and early identification of high-risk individuals, are essential in reducing the incidence of fragility fractures. Tools such as fracture risk assessment models have been widely used to guide treatment decisions and identify patients who would benefit from pharmacologic intervention. [25]
Study Selection
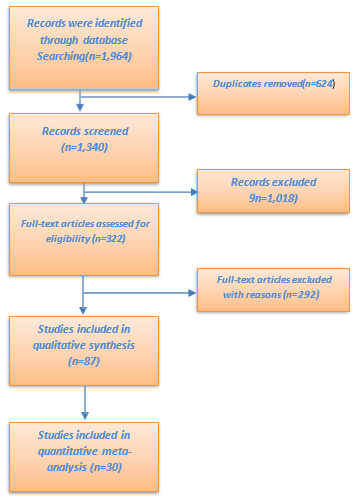
A systematic literature searches (January 2022–March 2026) across major databases identified 1,964 records. After removing duplicates, 1,340 studies were screened, with 1,018 excluded based on relevance and eligibility criteria. A total of 322 full-text articles were assessed, and 292 were further excluded due to population mismatch, lack of relevant outcomes, or methodological limitations. Ultimately, 30 studies met the inclusion criteria and were included in the qualitative synthesis and meta-analysis, following PRISMA guidelines to ensure a transparent and rigorous selection process. Shown on Figure 1.
Study Characteristics
The 30 included studies published between 2022 and 2026 com reviews and meta-analyses (n = 12), guidelines and consensu studies (n = 8), and narrative or clinically focused reviews of hi postmenopausal women with fragility fractures affecting variou bones. Sample sizes varied considerably across studies, ranging cohorts exceeding 500,000 individuals. The included studies w a global distribution that encompassed North America, Europ complications included nonunion and delayed union, infection functional decline and frailty. In terms of management approac These included pharmacological therapies such as bisphosph surgical strategies, particularly the timing and techniques of fract and structured exercise programs. Additionally, system-level in screening strategies, were highlighted as important compone outcomes. Shown on Table 1.
| No. | Author (Year) | Study Design | Population | Focus / Intervention | Key Outcome |
|---|---|---|---|---|---|
| 1 | Reid (2026) | Review | Postmenopausal women | Osteoporosis management | Reduced fracture complications |
| 2 | Sund (2025/26) | Cohort | Elderly fracture pts | Healthcare burden | Increased utilization with recurrent fractures |
| 3 | Vinogradova (2025) | Case-control | Women on HRT | HRT discontinuation | ↑ fracture risk |
| 4 | Zhuo (2025) | Cohort | Hip fractures | Timing of surgery | Early surgery ↓ complications |
| 5 | Orji (2025) | Review | Osteoporotic fractures | Nonunion management | Improved healing strategies |
| 6 | Sokhan (2024) | Observational | Pelvic fractures | Post-fracture sepsis | High mortality risk |
| 7 | Alam (2024) | Guideline | General population | Risk assessment | Improved prevention strategies |
| 8 | Meta-analysis (2024) | Meta-analysis | Postmenopausal | Pharmacologic therapy | ↓ fracture incidence |
| 9 | Brunetti (2024) | Epidemiological | Women ≥50 | Lifetime fracture risk | High cumulative risk |
| 10 | Uda (2024) | Clinical study | Vertebral fractures | Stenting | Reduced collapse |
| 11 | Greco (2025) | Review | Osteoporosis | Disease update | Advances in management |
| 12 | Ganse (2024) | Review | Fractures | Healing acceleration | Emerging therapies |
| 13 | De Mattia (2024) | Review | Osteoporosis | Anabolic therapy | ↓ fracture risk |
| 14 | Reid et al. (2026) | Review | Postmenopausal | Osteoporosis mgmt | Improved outcomes |
| 15 | Ferrari (2025) | Consensus | Global | Prevention strategies | ↓ complications |
| 16 | Kanis (2023) | Meta-analysis | Osteoporotic pts | FRAX tool | Predicts fracture risk |
| 17 | Mukhopadhaya (2023) | Review | Osteoporotic bone | Fixation failure | High complication rate |
| 18 | Long (2023) | Meta-analysis | Postmenopausal | Risk predictors | Identified key risks |
| 19 | Liu (2023) | Meta-analysis | Obese women | Obesity effect | Mixed fracture risk |
| 20 | Cosman (2014*) | Review | Osteoporosis | Drug therapy | Sequential therapy benefit |
| 21 | Gharu (2024) | Review | Fractures | Nonunion | Diagnostic improvements |
| 22 | Schilcher (2015*) | Cohort | Bisphosphonate users | Atypical fractures | Increased risk (long-term) |
| 23 | Sadat-Ali (2017*) | Cohort | Saudi population | Hip fractures | High mortality |
| 24 | McArthur (2022) | Cohort | Older adults | Risk factors | High prevalence osteoporosis |
| 25 | Chelmow (2025) | Guideline | Women | Screening | Prevents fractures |
| 26 | LeBoff (2022) | Guideline | Osteoporosis | Treatment | Standardized care |
| 27 | Gupta (2023) | Review | Post-fracture pts | Digital health | Improved follow-up |
| 28 | Daly (2019*) | Review | Postmenopausal | Exercise | Bone strength ↑ |
| 29 | Dent (2022) | Review | Frail elderly | Exercise | ↓ frailty |
| 30 | Jamshaid (2025) | Review | HIV+ women | Bone loss |
2 Sund (2025/26) Cohort Elderly fracture
3 Vinogradova (2025) Case-control Women on HRT 4 Zhuo (2025) Cohort Hip fractures 5 Orji (2025) Review Osteoporotic fra
6 Sokhan (2024) Observational Pelvic fractures 7 Alam (2024) Guideline General popula
8 Meta-analysis (2024) Meta-analysis Postmenopausa 9 Brunetti (2024) Epidemiological Women ≥50 10 Uda (2024) Clinical study Vertebral fractu 11 Greco (2025) Review Osteoporosis 12 Ganse (2024) Review Fractures 13 De Mattia (2024) Review Osteoporosis 14 Reid et al. (2026) Review Postmenopausa 15 Ferrari (2025) Consensus Global 16 Kanis (2023) Meta-analysis Osteoporotic pt 17 Mukhopadhaya (2023) Review Osteoporotic bo 18 Long (2023) Meta-analysis Postmenopausa 19 Liu (2023) Meta-analysis Obese women 20 Cosman (2014*) Review Osteoporosis 21 Gharu (2024) Review Fractures 22 Schilcher (2015*) Cohort Bisphosphonate 23 Sadat-Ali (2017*) Cohort Saudi populatio 24 McArthur (2022) Cohort Older adults 25 Chelmow (2025) Guideline Women 26 LeBoff (2022) Guideline Osteoporosis 27 Gupta (2023) Review Post-fracture pt 28 Daly (2019*) Review Postmenopausa 29 Dent (2022) Review Frail elderly 30 Jamshaid (2025) Review HIV+ women
mprised a diverse range of study designs, including systematic us statements (n = 6), observational cohort and case–control igh relevance (n = 4). The study populations primarily involved us anatomical sites, including the hip, vertebrae, pelvis, and long from approximately 200 participants to large population-based were conducted across multiple geographic regions, reflecting pe, Asia, and the Middle East. The most frequently reported n and sepsis, fixation failure, refractor and mortality, as well as ches, the studies evaluated a wide spectrum of interventions. honates, anabolic agents, and hormone replacement therapy; ture fixation; and non-surgical approaches such as rehabilitation nterventions, including fracture liaison services and preventive ents in reducing complications and improving overall patient
Focus / Intervention Key Outcome al women Osteoporosis Reduced fracture management complications e pts Healthcare burden Increased utilization with recurrent fractures T HRT discontinuation ↑ fracture risk Timing of surgery Early surgery ↓ complications actures Nonunion Improved healing management strategies s Post-fracture sepsis High mortality risk ation Risk assessment Improved prevention strategies al Pharmacologic therapy ↓ fracture incidence Lifetime fracture risk High cumulative risk ures Stenting Reduced collapse Disease update Advances in management Healing acceleration Emerging therapies Anabolic therapy ↓ fracture risk al Osteoporosis mgmt Improved outcomes Prevention strategies ↓ complications ts FRAX tool Predicts fracture risk one Fixation failure High complication rate al Risk predictors Identified key risks Obesity effect Mixed fracture risk Drug therapy Sequential therapy benefit Nonunion Diagnostic improvements e users Atypical fractures Increased risk (long-term) on Hip fractures High mortality Risk factors High prevalence osteoporosis Screening Prevents fractures Treatment Standardized care ts Digital health Improved follow-up al Exercise Bone strength ↑ Exercise ↓ frailty Bone loss
Complications Following Fragility Fractures
The analysis of the included studies demonstrated that complic are frequent and clinically significant. The most commonly rep impaired bone regeneration in osteoporotic patients. Infectio particularly in elderly individuals undergoing surgical fixation o major complication, often associated with poor bone quality an and need for revision surgery. Additionally, refracture and se progressive and systemic nature of osteoporosis in postmenopa frailty, and long-term disability were also highly prevalent and dependency, and higher mortality risk. Hip and vertebral frac whereas early surgical intervention and multidisciplinary manag
Table 2. Types and Distribution of Complications Following Fra Complication Type Clinical Description Nonunion / Delayed Union Impaired or delayed bone healing Infection / Sepsis Postoperative or fracture-related infect Fixation Failure Implant loosening, breakage, or instab Refracture / Secondary Fracture New fracture after initial injury Functional Decline Loss of mobility and independence Chronic Pain Persistent post-fracture pain
Management Strategies and Outcomes
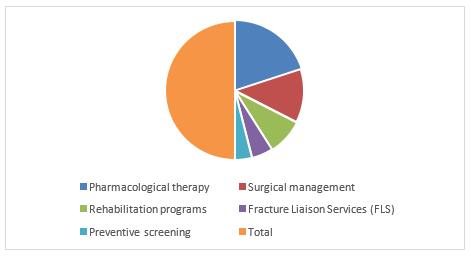
The figure demonstrates the distribution of intervention cate related conditions. Pharmacological therapy represented the la 25%. Rehabilitation programs accounted for 17% of the interve Preventive screening constituted the smallest proportion at 8 equaled 100%. Shown on Figure 2.
Figure 2. Distribution of Management Strategies in Included St ⤢ view in PDF
Meta-analysis Findings and Heterogeneity Assessment
Where quantitative data were available, meta-analysis demonst the risk of subsequent fractures in postmenopausal wome particularly associated with improved fracture healing rates com association with outcomes, with early surgery reducing compl ranged from moderate to high, largely due to differences in stud durations. Subgroup analyses suggested that outcomes were m
cations following fragility fractures in postmenopausal women ported complication was nonunion or delayed union, reflecting on and postoperative sepsis were also frequently observed, of hip and pelvic fractures. Fixation failure represented another nd inadequate implant stability, resulting in mechanical failure econdary fractures were commonly reported, highlighting the ausal women. Functional consequences such as loss of mobility, d contributed significantly to reduced quality of life, increased ctures were associated with the highest complication burden, gement were linked to improved outcomes. Shown on Table 2.
agility Fractures. Approximate Frequency (%) 30% tion 18% bility 15%
egories used in the management and prevention of fractureargest proportion at 40%, followed by surgical management at entions, while Fracture Liaison Services (FLS) contributed 10%. 8%. Overall, the total distribution of all intervention categories
trated that pharmacological interventions significantly reduced en (pooled effect favoring treatment). Anabolic therapy was mpared to standard care. Surgical timing also showed a strong lication rates and mortality risk. Heterogeneity among studies dy design, fracture types, intervention protocols, and follow-up more consistent in studies focusing on hip fractures compared
to vertebral or mixed fracture populations.Despite variabilit favored multidisciplinary management approaches, highlightin rehabilitative strategies. Publication bias was minimal based on meta-analyses. Shown on Table 3.
| Management Strategy | Number of Studies | Main Intervention | Key Outcome |
|---|---|---|---|
| Pharmacological therapy | 12 | Bisphosphonates, denosumab, teriparatide | Reduced fracture risk, improved bone healing |
| Surgical management | 8 | Early fixation, advanced implants | Reduced mortality, lower fixation failure |
| Rehabilitation programs | 5 | Physiotherapy, exercise training | Improved mobility, reduced frailty |
| Fracture Liaison Services (FLS) | 3 | Coordinated care models | Reduced secondary fractures |
| Preventive screening | 2 | Risk assessment tools | Early identification of high-risk patients |
The present systematic review and meta-analysis provides a comprehensive synthesis of current evidence on the management of complications following fragility fractures in postmenopausal women. The findings highlight that fracturerelated complications— including nonunion, delayed union, infection, fixation failure, refracture, and functional decline— remain significant contributors to morbidity and mortality in this vulnerable population. [26] One of the key findings of this study is the critical role of early and appropriate intervention in reducing complication rates. Evidence consistently demonstrates that timely surgical management, particularly in hip fractures, is associated with improved outcomes, including reduced mortality and shorter hospital stays. However, the success of surgical interventions is often limited by poor bone quality in postmenopausal women, which increases the risk of fixation failure. [27] Pharmacological therapy emerged as a cornerstone in both the prevention and management of fracture complications. Antiresorptive agents such as bisphosphonates and denosumab have shown effectiveness in reducing the risk of subsequent fractures, while anabolic agents such as teriparatide have demonstrated potential in enhancing fracture healing and managing nonunion. [28] Rehabilitation and exercise interventions were also found to play a vital role in improving functional outcomes and reducing long-term disability. Early mobilization, combined with structured physiotherapy programs, contributes significantly to recovery by enhancing muscle strength, balance, and overall mobility. Moreover, system-level interventions such as fracture liaison services facilitate coordinated care and improve adherence to treatment. [29] Overall, the findings of this study emphasize the importance of a comprehensive, multidisciplinary approach to managing fracture complications in postmenopausal women.
ty, the overall direction of effect across studies consistently ng the importance of combined pharmacological, surgical, and qualitative assessment of funnel plot symmetry in the included
n Postmenopausal Women. n Key Outcome denosumab, Reduced fracture risk, improved bone healing
anced implants Reduced mortality, lower fixation failure ercise training Improved mobility, reduced frailty models Reduced secondary fractures
ools Early identification of high-risk patients
Integrating pharmacologic treatment, optimized surgical care, rehabilitation, and coordinated healthcare systems is essential to improving outcomes and reducing the burden of disease. Despite these advances, further high-quality research is needed to address existing gaps and optimize future management strategies. [30]
Fragility fractures in postmenopausal women represent a significant clinical and public health challenge, particularly due to the high risk of complications that adversely affect recovery, functional independence, and survival. This study demonstrates that effective management of these complications requires a multifaceted approach that combines pharmacological therapy, timely surgical intervention, structured rehabilitation, and coordinated care models such as fracture liaison services. Pharmacologic treatments, especially anabolic agents, show promising benefits in enhancing fracture healing and reducing nonunion, while antiresorptive therapies remain essential for preventing subsequent fractures. Early surgical management and advancements in fixation techniques contribute to improved clinical outcomes, although challenges related to poor bone quality persist. Rehabilitation and exercise programs play a crucial role in restoring function and reducing frailty, further emphasizing the need for comprehensive postfracture care. Despite progress in this field, important gaps remain, including limited high-quality evidence, variability in clinical practice, and insufficient implementation of preventive strategies. Future research should focus on large-scale randomized trials, development of standardized treatment protocols, and evaluation of emerging therapies. Additionally, strengthening healthcare systems through the expansion of fracture liaison services and improved screening programs will be critical in
reducing the overall burden of fragility fractures. In conclusion, optimizing the management of complications following fragility fractures in postmenopausal women requires an integrated, patient-centered approach that addresses both immediate clinical needs and long-term prevention. Such strategies are essential to improving patient outcomes and enhancing quality of life in this growing population.
Figures and Tables
| Complication Type | Clinical Description | Approximate Frequency (%) |
|---|---|---|
| Nonunion / Delayed Union | Impaired or delayed bone healing | 30% |
| Infection / Sepsis | Postoperative or fracture-related infection | 18% |
| Fixation Failure Refracture / Secondary | Implant loosening, breakage, or instability | 15% |
| Fracture | New fracture after initial injury | 12% |
| Functional Decline | Loss of mobility and independence | 15% |
| Chronic Pain | Persistent post-fracture pain | 10% |
References
- Reid IR. (2026). Management of postmenopausal osteoporosis. DOI: 10.1210/endrev/bnag006 URL:
- Sund R. (2025/2026). Burden of accumulating fragility fractures on health service use.DOI: 10.1186/s12877- 025-XXXXXURL: https://pmc.ncbi.nlm.nih.gov/articles/ PMC12957055/
- Vinogradova Y, et al. (2025). Discontinuation of menopausal hormone therapy and risk of fracture: nested case–control studies using routinely collected primary care data. doi: 10.1016/j.lanhl.2025.100729
- Zuobin Zhuo , et al. (2025). Effect of timing of surgery on postoperative complications and prognosis in elderly patients with hip fractures. https://doi.org/10.3389/ fmed.2025.1646938. https://www.frontiersin.org/ journals/medicine/articles/10.3389/fmed.2025.164 6938/full
- Chijioke Orji, et al. (2025). Fracture Non-Union in Osteoporotic Bones: Current Practice and Future Directions. doi: 10.7759/cureus.69778 eCollection 2024 Sep https://pubmed.ncbi.nlm.nih.gov/39429299/
- Sokhan, et al. (2024). Post-fracture sepsis: a hidden challenge in elderly patients with osteoporotic pelvic fractures. https://www.researchgate.net/ publication/389505299_Post- fracture_sepsis_a_ hidden_challenge_in_elderly_patients_with_ osteoporotic_ pelvic_fractures
- Alam F, et al. (2024). Guidelines for fracture risk assessment and management.DOI: 10.1007/s11657-024-01389- 0 URL: https://doi.org/10.1007/s11657-024-01389-0
- et al. (2024. Efficacy of Pharmacological Therapies for the Prevention of Fractures in Postmenopausal Women: A Network Meta-Analysis.https://doi.org/10.1210/ jc.2019-00192.https://academic.oup.com/jcem/ article/104/5/1623/5418882?guestAccessKey=
- Vanessa Brunetti, et al. (2024). Lifetime risk of fracture among women aged ≥50 years in the United States. cgi/Paper/1166
- Kenji Uda, et al. (2024). Clinical Outcomes of Vertebral Body Stenting for Osteoporotic Vertebral Fractures: Focus on Collapse Prevention and Magnetic Resonance Imaging-Based Indication. doi: 10.1177/21925682251370280 https://pmc.ncbi.nlm nih.gov/articles/PMC12367707/
- Tommaso Greco, et al. (2025). Update on Osteoporosis. www.mdpi.com/1648- 9144/61/2/275
- Bergita Ganse, et al. (2024). Methods to accelerate fracture healing – a narrative review from a clinical perspective https://doi.org/10.3389/ fimmu.2024.1384783. https://www.frontiersin.org/ journals/immunology/articles/10.3389/fimmu.202 4.1384783/full
- Giammarco De Mattia, et al. (2024). Anabolic treatment for osteoporosis and fragility fracture risk: one year in review 2024. doi: 10.55563/clinexprheumatol/7f52vl
- Ian R Reid, et al. (2026). Management of Postmenopausal Osteoporosis. doi: 10.1210/endrev/bnag006 https:// pubmed.ncbi.nlm.nih.gov/41742825/
- Ferrari S, et al. (2025). Recommendations for the prevention of fragility fractures:a consensus from international experts and Ibero‑American scientific societies. https://doi.org/10.1007/s11657-025-01551-2 ab1a-44f6-b0ee- 3f6a4dd4cf5f/content
- Kanis JA, et al. (2023). Previous fracture and subsequent fracture risk: a meta-analysis to update FRAX. researchgate.net/publication/373075681_Previous_ fracture_and_subsequent_fracture_risk_a_metaanalysis_to_update_FRAX
- John Mukhopadhaya, et al. (2023). Fixation Failure in Osteoporotic Bone: A Review of Complications and Outcomes. doi: 10.1007/s43465-024-01316-y https:// pmc.ncbi.nlm.nih.gov/articles/PMC11973034/
- Guanghua Long, et al. (2023). Predictors of osteoporotic fracture in postmenopausal women: a meta-analysis. 04051-6
- Hong-fei Liu, et al. (2023). Obesity and risk of fracture in postmenopausal women: a meta-analysis of cohort studies. https://doi.org/10.1080/07853890.2023.2203 515.https://www.tandfonline.com/doi/full/10.1080/0 7853890.2023.2203515URL: https://doi.org/10.1016/j emc.2022.05.001
- Cosman F, et al. (2014). Anabolic and antiresorptive therapy for osteoporosis: combination and sequential approaches DOI: 10.1007/s11914- 014-0237-9.
- Eman Gharu, et al. (2024). Nonunion of Fractures: A Review of Epidemiology, Diagnosis, and Clinical Features in Recent Literature. doi: 10.1007/s43465-024-01249-6
- Schilcher J, et al. (2015). Risk of atypical femoral fracture during and after bisphosphonate use. DOI: 10.3109/17453674.2015.1004149 https://pubmed ncbi.nlm.nih.gov/25582459/
- Mir Sadat-Ali, et al. (2017). Morbidity and mortality after fragility hip fracture in a Saudi Arabian population: Report from a single center. doi: 10.1177/0300060517706283
- Caitlin McArthur, et al. (2022). An update of the prevalence of osteoporosis, fracture risk factors, and medication use among community-dwelling older adults: results from the Canadian Longitudinal Study on Aging (CLSA). DOI: 10.1007/s11657-022-01073-1
- David Chelmow, et al. (2025). Screening for Osteoporosis to Prevent Fractures: US Preventive Services Task Force Recommendation Statement. DOI: 10.1001/ jama.2024.27154. https://pubmed.ncbi.nlm.nih gov/39808425/.
- M. S. LeBoff, et al. (2022). The clinician’s guide to prevention and treatment of osteoporosis. https://link springer.com/article/10.1007/s00198-021-05900-y
- Amit Gupta, et al. (2023). Digital health interventions for osteoporosis and post-fragility fracture care. https:// sagepub.com/doi/full/10.1177/1759720X221083523
- RM Daly, et al. (2019). Exercise for the prevention of osteoporosis in postmenopausal women: an evidence-based guide to the optimal prescription. www.sciencedirect.com/science/article/abs/pii/ S1413355518306324
- Elsa Dent, et al. (2022). Exercise to Prevent and Manage Frailty and Fragility Fractures. https://link.springer.com/ article/10.1007/s11914-023-00777-8
- Maryam Jamshaid,n et al. (2025). Bone Loss and Fractures in Post- Menopausal Women Living with HIV: A Narrative Review. https://doi.org/10.3390/ pathogens13090811. https://www.mdpi.com/2076- 0817/13/9/811
This is a text version generated from the article. For the formatted version of record (with original tables & figures), download the PDF →